Computer-aided detection (CAD) is sensitive for all but the flattest of flat colorectal lesions, even in minimally prepped patients, according to a new study from Italy. Using CAD, radiologists significantly improved their ability to detect the elusive polyps, which can harbor precancerous lesions.
Virtual colonoscopy (also known as CT colonography or CTC) can detect flat lesions in the colon. However, flat polyps that are only superficially elevated above the colonic mucosa can potentially be difficult to detect when they are 1-2 mm or less in elevation, authors from the University of Rome "La Sapienza" concluded.
Suboptimal distention of a colonic segment can further reduce sensitivity for flat lesions, which are also sometimes missed in conventional colonoscopy, especially when performed without mucosal staining, which is rare in U.S. gastroenterology practices.
 |
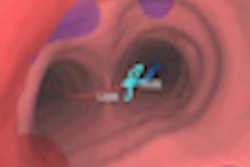
| Six lesions located on haustral folds showed higher conspicuity in 3D versus 2D renderings. In particular, focal thickening and surface irregularities were more visible at 3D. All images courtesy of Dr. Franco Iafrate. |
 |
The use of CAD, either concurrently or as a second reader, improves detection of sessile and polypoid lesions 6 mm and larger. But little is known of CAD's performance in morphologically flat lesions, and the issue needs further study, said Dr. Franco Iafrate at the 2009 RSNA meeting in Chicago.
In addition to the lack of information about CAD's performance with flat polyps, "we know there is some controversy regarding the prevalence, the clinical importance, and appropriate screening methods for nonpolypoid polyps of the colon," he said.
Their study aimed to evaluate the ability of CAD software (im3D, Turin, Italy) to detect morphologically flat lesions at CT colonography.
The CTC data consisted of 31 patients with 34 endoscopically proven flat lesions. Of these, 11 were undergoing polyp surveillance follow-up, seven patients had a family or personal history of colorectal polyps or cancer, and 13 were asymptomatic screening subjects considered to be at average risk of the disease, Iafrate said.
The CTC data were evaluated in consensus by three expert readers who were unaware of the endoscopic results.
A total of 28/31 patients underwent only a fecal tagging prep before CTC, which consisted of ingesting 70 mL of iodinated oral contrast media. The remaining three patients underwent a full cathartic prep. The group measured mean reading time using a primary 2D approach with 3D as a problem-solving tool.
Both with and without the use of CAD as a second reader, they assessed sensitivity, false positives in both prone and supine scanning, and the rate of correct localization of lesions between the two modalities.
The 34 endoscopically proven polyps included:
- 19 lesions 3 mm in height
- 11 lesions 1-3 mm in height
- Two lesions < 2 mm in height
- Three lesions more than three times higher than wide
The team found that CAD improved the sensitivity of the radiologists who used it compared to radiologists without CAD: 26 of 34 lesions (76%) were detected by radiologists alone without CAD, compared to 30 of 34 (88%) lesions detected by the radiologists using CAD.
But radiologists working with CAD did not achieve the sensitivity of CAD alone, with 32 of 34 (94%) lesions detected by CAD on its own. This is because radiologists working with CAD dismissed some true-positive CAD findings, Iafrate said.
Four of 34 lesions were located in the transverse colon, 13 in the ascending colon, 11 in the cecum, four in the descending colon, and two in the rectum. Two lesions less than 1 mm in height weren't seen at CTC and were difficult to discern even retrospectively.
Six polyps located on the haustral fold showed higher conspicuity on the 3D endoluminal view than on the 2D view (colon window setting), Iafrate said.
As for histology, 22 of 34 lesions were adenomas with low-grade dysplasia and 24 of 34 were located within the right colon. Eight of 34 flat lesions showed severe dysplasia, two of 34 were flat cancers (maximum diameter 3.5 cm, detected by CAD and the radiologists), and two of 34 were hyperplastic.
Two lesions were detected only by CAD and were not reported by the radiologists as flat due to low conspicuity. Two lesions with heights < 1 mm weren't seen at CTC but were detected at conventional colonoscopy.
 |
| Two lesions showing a typical cigarlike appearance were detected only by CAD and were not reported by the radiologists as flat due to low conspicuity. Left to right: 2D image, 3D endoscopic view, colonoscopy view. |
 |
| Two lesions with heights < 1 mm weren't seen at CTC despite optimal technology. Above, "carpet" lesion not visualized at CTC. |
Reading time was much faster with the use of CAD: four minutes, 28 seconds, with 2D plus 3D interpretation, versus 52 seconds using CAD, Iafrate said.
"From our little cohort of patients with flat lesions, probably 25% were missed by radiologists without CAD, and CAD seems to improve lesion detection from 75% to 90% in those patients," Iafrate said. "CT colonography can detect flat lesions in the colon; however, flat polyps that are superficially elevated can be difficult to detect, [especially] when they are 1-2 mm in elevation."
The main limitation of the study is probably that patients were selected for it based on the known presence of flat lesions, he said.
An audience member commented that it could be difficult, especially for less experienced readers, to dismiss false-positive CAD marks located on haustral folds. Another was surprised at the high rate of adenomas, which, at 22/34 flat lesions in the cohort, represented a far higher rate than seen in previous studies.
By Eric Barnes
AuntMinnie.com staff writer
December 16, 2009
Related Reading
ACRIN: Virtual colonoscopy sensitive for flat polyps, October 13, 2009
Flat-polyp measurements show less variability in 3D VC, September 16, 2009
Virtual colonoscopy CAD improves flat-lesion detection, June 5, 2009
ACRIN trial shows VC accuracy comparable to optical colonoscopy, September 18, 2008
Minimal-prep VC may miss more flat lesions, April 17, 2008
Copyright © 2009 AuntMinnie.com