SAN FRANCISCO - One of the largest CT studies to date of acute appendicitis has confirmed the modality's sky-high diagnostic accuracy. The results, unveiled on Wednesday at the International Society for Computed Tomography (ISCT) meeting, also showed that CT is relatively insensitive to imaging technique, though the researchers said they have come to favor the use of oral contrast.
"I don't think I have to convince you that acute appendicitis is an important clinical problem. The lifetime risk is about 7% to 8%, and it's as much an adult disease as it is children only, with a median age of 22 years and a mean age that is considerably higher," said Dr. Perry Pickhardt, professor of Radiology at the University of Wisconsin in Madison.
For its part, MDCT, the imaging method of choice for acute appendicitis, delivers diagnostic performance that is generally well established, with pooled sensitivity and specificity exceeding 95% in older studies.
In the more recent multislice era, there are less data on accuracy and more on utilization, Pickhardt said; other trends include the increasing use of MRI and ultrasound in certain groups such as pregnant and pediatric patients.
As for the older CT studies, Rao et al in 1998 had only 100 patients, but their study showed a remarkable rate of management change in nearly half the cases after CT, Pickhardt said. Flum and colleagues countered in 2001 with conflicting data showing no change in the negative appendectomy rate with CT, but the imaging utilization rate was unknown and probably quite low in that single-slice CT series, he said.
And at least three other studies covering the period between 2000 and 2006 (including Raman et al, 2008, and Coursey et al, 2010) with a prevalence of at least 20% confirmed that the negative appendectomy rate dropped from more than 20% to less than 10% with the use of CT, Pickhardt said.
"One thing that's lacking is the actual diagnostic performance or accuracy with MDCT ... so we looked at what I think is the largest CT-based cohort for appendicitis," a total of 1,666 adults with suspected acute appendicitis between 2000 and 2006, Pickhardt said.
The prevalence of disease was 24.4% (20.8% women, 32.6% men), Pickhardt said, but other than that no diagnostic differences between the men and women were apparent. MDCT's diagnostic performance in the cohort was as follows:
- Sensitivity = 98.0%
- Specificity = 98.2%
- Negative predictive value = 99.4%
- Positive predictive value = 94.5%
- Accuracy = 98.1%
- Area under the receiver operator characteristics (ROC) curve = 0.995 ± 0.0016
"We were very pleased to see that sensitivity, specificity, and accuracy were all over 98%, with high predictive values as well" Pickhardt said.
"Our negative appendectomy rate was under 10% as the other studies have shown, but, interestingly, it would have been under 4% had 21 cases that were negative for CT not gone on to appendectomy," he said. "I think it goes to show that in some cases we should really stick to our guns and trust our instincts."
 |
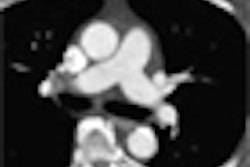
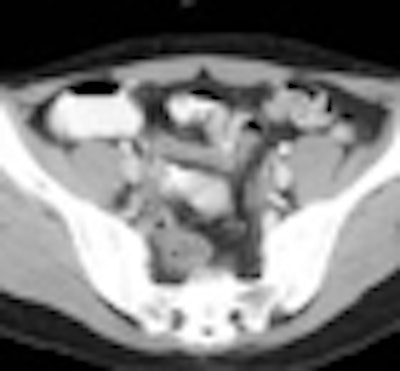
| Tumors can cause obstructive appendicitis, especially in elderly populations, as in the cecal cancer, above, causing acute appendicitis. Below, alternative diagnosis of an intussuscepted appendicele. All images courtesy of Dr. Perry Pickhardt. |
 |
Diagnosing acute appendicitis
MDCT signs also well established include appendiceal (enlargement [> 6-10 mm], wall thickening [≥ 3 mm], hyperenhancement, fluid-filled lumen, appendicolith) and periappendiceal (stranding fascial thickening fluid, phlegmon, abscess) findings.
"The most important findings are wall thickening, hyperenhancement of the thickened wall, unopacified fluid filling, and, of course, periappendiceal stranding is highly useful," Pickhardt said. "Many of these findings actually require oral and/or IV contrast, and I've come full circle to really think that to fully optimize accuracy, we need to maintain a positive oral contrast regimen and a nonfocused technique."
In fact, that's the ongoing debate, he said. Do you perform a contrast exam, a noncontrast exam, or somewhere in between?
Pickhardt believes that oral contrast helps ensure the correct diagnosis. Typically, MDCT shows a thickened, enhancing wall, and a nonopacified lumen. Without oral contrast, the diagnosis can easily hinge on the periappendiceal findings, he said. In other cases, the presence of the arrowhead sign or the cecal bar sign indicates the presence of cecal apical edema, another sign of acute appendicitis that can seal the diagnosis, Pickhardt said, adding that MDCT is usually able to make the diagnosis even when the technique isn't optimal.
"In the end, nearly any MDCT protocol works," he said.
"The use of oral and IV contrast really helps in difficult cases," Pickhardt said. "You can certainly get away with no contrast and actually do quite well; the question is, do you want to do a few points better, and I'm a proponent of [doing] more than a general scan of the abdomen and pelvis."
It's also everyone's job to work on reducing the dose, he said, which is easy enough as the appendix is so well visualized at minimal doses. The use of multiplanar reconstruction can improve the visualization and should be used routinely, he said.
"MDCT is the gold standard for suspected acute appendicitis in adults," he said. "It's highly accurate, it's efficient, it's now highly utilized as a preoperative imaging tool in almost all cases, and it's relatively resistant to technique, although I do favor positive oral and IV contrast. Lower dose is the next frontier."
By Eric Barnes
AuntMinnie.com staff writer
May 20, 2010
Related Reading
Preoperative CT may reduce negative appendectomies in women, January 28, 2010
Noncontrast CT accurately diagnoses acute appendicitis in adults, January 25, 2010
Limit CT exams for appendicitis in kids, November 24, 2009
CT coronal reconstructions aid pediatric appendicitis diagnosis, January 12, 2009
Feel-good CT-positive appendicitis cases rarely elude surgery, January 12, 2009
Copyright © 2010 AuntMinnie.com