Advanced imaging for the diagnosis of acute pancreatitis (AP) is overused, according to a study published online in Radiology from researchers at Brigham and Women's Hospital in Boston. They found that clinical assessment of acute pancreatitis, rather than advanced imaging, works just fine for most patients.
The researchers assessed imaging use trends for acute pancreatitis and independent predictors of radiology use in relation to patient outcomes (Radiology, October 27, 2010). Using acute pancreatitis to track the use of advanced imaging is helpful, according to lead author Koenraad Mortele, MD, and colleagues, as it accounts for more than 220,000 annual hospital admissions in the U.S.
"Studying imaging utilization in patients with AP is appealing because of the high estimated total healthcare cost associated with the disease, the presence of well-established practice guidelines for managing the disease, and the vast array of radiologic modalities that are available to image these patients," they wrote.
For the study, Mortele's team included all 252 adult patients admitted to the hospital with a diagnosis of acute pancreatitis between June 2005 and December 2007. Patients who had been transferred from other hospitals or those with a history of chronic pancreatitis were not included. The group defined acute pancreatitis as two or more of the following characteristics:
- Severe upper abdominal pain
- Serum amylase and/or lipase levels three or more times higher than normal
- CT or MR imaging results that demonstrated changes consistent with AP
With the hospital's radiology database, the researchers also identified all acute pancreatitis-related imaging studies for each patient, classifying them according to modality and technique. The team also applied the U.S. Centers for Medicare and Medicaid Services (CMS) 2009 relative value units (RVUs) for each study to have a consistent scale with which to assess differences across exam types.
A total of 1,324 radiologic studies were performed during the study time frame. During initial hospitalization, the mean imaging utilization rate was 5.3 studies per patient, with an RVU of 3.9; in the one-year period after the initial admission, the mean utilization rate was 9.9 exams per patient, with an RVU of 7.8. Overall, 53% of the total imaging use occurred during a patient's initial hospitalization.
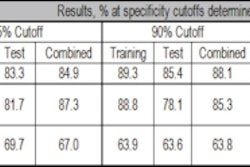
The most common exams included chest radiography, abdominal CT, pelvic CT, and abdominal ultrasound. Imaging use by modality during the one-year period following initial hospitalization is detailed in the following chart:
Imaging use by modality for acute pancreatitis
|
||||||||||||||||||||||||
| Data courtesy of the Radiological Society of North America. |
The team found a 2.5-fold increase in the use of high-cost radiologic examinations for acute pancreatitis and a 1.4-fold increase in imaging RVUs (per case-mix-adjusted admissions) during the study period -- without noticeable improvement in patient outcomes. (Improvement in patient outcomes was measured with mortality, admission to intensive care units, need for surgery, organ failure, or presence of persistent systemic inflammatory response syndrome.)
"In this analysis, patient outcomes were relatively stable during the study period. ... Therefore, although it remains difficult to analyze the effect of imaging utilization on patient outcomes, it can probably be inferred that in our institution the increasing use of cross-sectional imaging did not result in detectable improvement in outcomes for patients with AP," the authors wrote.
The team was surprised to find that even though 90% of the patients in the study had mild disease, CT and MR use surpassed what is recommended by the American College of Radiology's Appropriateness Criteria. This occurred despite the fact that there is no information in existing literature that suggests that CT scans in patients with milder disease would result in upstaging of disease in a significant number of patients, according to the researchers.
And there's no advantage to performing early imaging to predict the clinical severity of acute pancreatitis rather than just using a clinical evaluation, they noted.
"If a diagnosis of AP is established with abdominal pain and increased serum amylase and lipase activity and no systemic signs of severe disease exist, CT may not be necessary," Mortele and colleagues wrote.
Instead, CT should be reserved for patients with an equivocal diagnosis, those who have already been established as having severe acute pancreatitis, or those who don't improve despite conservative measures, they concluded.
By Kate Madden Yee
AuntMinnie.com staff writer
November 9, 2010
Related Reading
Leaders in Imaging: A conversation with William Hendee, PhD, October 13, 2010
Radiologists call for curbs on overuse of imaging, August 24, 2010
CMS unveils imaging decision-support initiative, July 23, 2010
One-quarter of outpatient CT and MRI exams are inappropriate, March 1, 2010
CDC report: MRI, CT, PET use spikes in physician offices, ER, February 18, 2010
Copyright © 2010 AuntMinnie.com