Manually displacing breast tissue during coronary CT angiography (CTA) reduces radiation dose to the breast surface by almost a quarter -- and even more if lead shielding is added, according to a study published in the August issue of the American Journal of Roentgenology.
Dr. Shane Foley, of the University College Dublin, and colleagues found that mean breast surface dose was reduced by 23% in patients who had manual breast displacement and by 36% in those who also received lead shielding.
The study team had set out to evaluate the effect of breast displacement and lead shielding on breast surface radiation dose in women undergoing coronary CTA.
"Coronary CTA typically includes most of the breast tissue within its scan range, exposing the breasts to radiation even though the breast is not the target organ," Foley and colleagues wrote. "Displacing the breasts cranially outside the direct x-ray beam therefore has potential as a method of reducing radiation exposure to this organ ... [and] removing breast tissue from the scan range may also improve image quality."
Fifty-four women had coronary 64-MDCT angiography for evaluation of chest pain. The patients were randomly assigned to a control group (16 women), a breast displacement group (22 women), or a breast displacement plus lead shielding group (16 women). Those women in the two groups that used breast displacement manually moved the breast tissue themselves, and then a breast displacement system was wrapped around the chest wall (AJR, August 2011, Vol. 197:2, pp. 367-373).
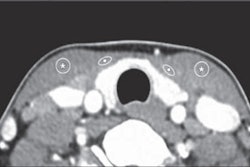
Thermoluminescent dosimeters (TLDs) were placed on each of the women's breast quadrants and the areolar region of each breast. A total of 1,620 TLD dose measurements were recorded.
Compared with the control group, the mean breast surface dose was reduced by 23% in the breast displacement group and 36% in the breast displacement plus lead shielding group (24.3 mGy versus 18.6 mGy, and 24.3 mGy versus 15.6 mGy, respectively).
Surface dose reductions were greatest in the upper outer (displacement alone: 66%, displacement plus shielding: 63%), upper inner (displacement alone: 65%, displacement plus shielding: 58%), and areolar quadrants (displacement alone: 44%, displacement plus shielding: 53%). Breast cup size affected the results: Women with smaller breasts had less dose reduction than those with larger breasts.
Foley's team did not note any significant difference in the quality of the coronary image between the two groups that used breast displacement.
"Breast displacement during coronary CTA is a feasible technique that results in a significant reduction in mean breast surface radiation dose without affecting coronary image quality," the authors concluded. "[Women with] larger breasts benefit most from the technique."