CHICAGO - Researchers have long known of differences between men and women in the rate of cardiac disease and resulting morbidity, but a new study presented at RSNA 2011 suggests that the same coronary CTA (CCTA) results require different interpretation and risk assessments depending on the patient's gender.
Looking at a cohort of nearly 500 chest pain patients with evidence of coronary artery plaque at dual-source CCTA, researchers from the Medical University of South Carolina (MUSC) found that men had more calcified and mixed plaque than women -- but that the calcifications were less dangerous in men than in women. Conversely, women had more noncalcified plaque than men, but it was less dangerous for them in terms of major adverse cardiac events.
"The point of the trial was to see the prognostic value associated with these findings, and we found that women with more than four coronary artery segments affected by plaque had nearly twice the risk as men," said Dr. John Nance, currently a radiology resident at Johns Hopkins, who performed the study at MUSC. Men had greater risk when they had noncalcified plaque, but women had a greater risk when they had calcified plaque.
It doesn't mean women have a greater risk of cardiac events than men, he added, but it "goes to show we need to consider what we find on coronary CTA between men and women differently," he said.
CCTA is an appropriate test in many cases of acute chest pain, especially in women who often have atypical presentations and in whom SPECT imaging is susceptible to breast attenuation artifacts, Nance said. Last year, he noted, Shaw and colleagues reported that the extent of nonobstructive (< 50% stenosis) coronary artery disease at CCTA holds incremental predictive value over obstructive burden in women but not men. However, the predictive value of CCTA characterization beyond the presence and extent of obstructive and nonobstructive disease is less well-established, particularly the prognostic value of specific morphological characterization.
The retrospective study aimed to determine the differences in the predictive value associated with various CCTA findings for the occurrence of major adverse cardiac events (MACE) between women and men presenting with acute chest pain but without acute coronary syndrome.
The group examined 2,682 charts of patients who underwent CCTA for investigation of chest pain. The 480 patients included in the study all had CCTA performed for acute chest pain with intermediate pretest probability of coronary artery disease. Full clinical and demographic data as well as follow-up data also had to be available, Nance said.
All patients underwent CCTA on a dual-source scanner (Somatom Definition, Siemens Healthcare) using 32 x 2 x 0.6-mm collimation, 0.2-0.5 pitch, 80-120 kV tube current, 350 mAs per rotation, reconstructions of 0.75 mm, and electrocardiogram (ECG) tube current modulation.
Demographic data were recorded on risk factors including hypertension, hypercholesterolemia, diabetes, age, hypertension, smoking status, body mass index (BMI), and Framingham risk score. "The average age was 55 years, and there were no significant differences in demographic parameters that we considered other than obesity," Nance said. "The women had higher BMI and greater rates of obesity than men, but no significant differences in smoking, hypercholesterolemia, or hypertension," he said.
Using a 15-segment American Heart Association model, the investigators looked for plaque, obstructive plaque (≥ 50% stenosis), and mixed and noncalcified plaque. The primary end point was a major adverse cardiac event, including cardiac death, nonfatal myocardial infarction, unstable angina, or revascularization (coronary artery bypass graft surgery or stenting).
During the follow-up period of 12.8 ± 7.0 months, 87 events occurred in 70 of the 480 patients, including three cardiac deaths, 13 myocardial infarctions, 33 revascularizations, and 38 cases of unstable angina, Nance reported. There were significant gender differences with respect to type and extent of plaque and stenosis between subjects with and without MACE (all p < 0.01).
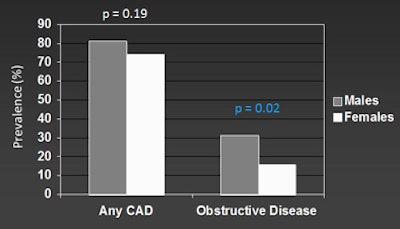
Among the 70 patients with MACE over the year-long follow-up, 38 were men (23%) and 32 were women (10%).
While there were more major cardiac events in men than women, the overall rates of coronary artery disease were about the same. "Women with more than four coronary artery segments affected by plaque had nearly twice the risk as men," Nance said. "In contrast, men had a greater risk when they had noncalcified plaque, while women had a greater risk when they had calcified plaque -- which was rarer in women and the noncalcified plaque was rarer in men."
 |
| All images courtesy of Dr. John Nance. |
 |
 |
| Different risks (hazard ratios) are associated with CCTA findings in men and women. |
In women, the risk associated with the presence of any plaque was significantly higher than in men (hazard ratio [HR]: 49.3 versus 39.1, p = 0.04 and 0.03) compared to patients with no plaque. The risk associated with four or more coronary segments with any plaque involvement was also higher in women than in men (HR: 113.9 versus 66.9, both p < 0.001) compared to patients with no plaque, he said. Importantly, each segment containing noncalcified plaque conferred a higher risk in men compared to women (HR: 2.2 versus 1.55, both p = 0.01).
Like a lot of other data coming out now, this study "points not only to individualized care for patients, but to individualized interpretation of their imaging studies," Nance said. "We have to consider their race, their sex, and everything else -- not only when we report findings, but when we report the significance of those findings."



















