Cocaine users are known to have higher-than-normal rates of acute coronary syndrome (ACS) compared to others at risk of heart disease. Researchers from the Medical University of South Carolina (MUSC) used dual-source CT to learn more about how cocaine use affects the development of coronary atherosclerosis.
Combing through an emergency department database, Dr. Hans Ebersberger and colleagues from MUSC as well as University Medical Center Groningen in the Netherlands found that cocaine use was associated with significantly greater prevalence of mixed-plaque coronary atherosclerosis, which is associated with ACS.
Cocaine use stresses the heart in several ways, Ebersberger explained last month in a presentation at the 2012 European Congress of Radiology (ECR).
"It can increase myocardial oxygen demand by increasing the heart rate, increasing the blood pressure as well as myocardial contractility," he said. "It also can lead to vasoconstriction due to increased alpha-adrenergic stimulation, increased endothelin production, and decreased nitric oxide production."
 |
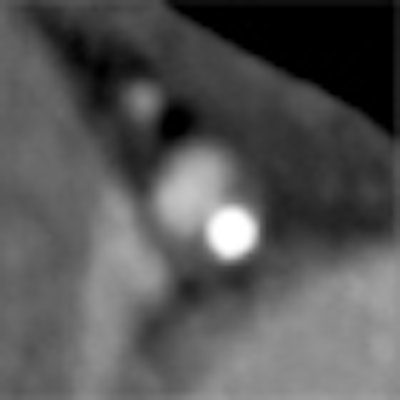
| Coronary CT angiography in cocaine user shows mixed plaque in the proximal left anterior descending artery. All images courtesy of Dr. Hans Ebersberger. |
Cocaine-associated chest pain accounts for a high proportion of emergency department visits in the U.S., he said; in fact, one-fourth of all acute myocardial infarction cases in patients 18 to 45 years old have been linked to use of the drug.
But even though the overall prevalence of noncalcified and calcified plaque in cocaine users has been found equal to that of age- and gender-matched controls, little is known about plaque distribution, he said.
"The prevalence of different plaque types, and especially mixed plaques, is largely unknown, so the purpose of our study was to evaluate possible differences in plaque burden and composition, and also degree of stenosis in cocaine users presenting to the emergency department," Ebersberger said.
The retrospective cohort study included 932 patients presenting to the emergency department between 2008 and 2011 with acute chest pain. A chart review identified 68 patients (48 men; median age, 44 years ± 6.9) with a history of cocaine abuse, including 18 under acute influence of the drug in the emergency room who underwent coronary CT angiography.
Sixty-eight patients with nonoccasional cocaine use (at least three times per year) were matched and compared in a 1-to-1 ratio to nonusers by race, gender, age, and risk factors (diabetes, hypertension, hyperlipidemia, smoking, family history, etc.).
All coronary CT angiography scans were performed on a dual-source scanner (Somatom Definition or Definition Flash, Siemens Healthcare). The group evaluated each coronary artery segment for the presence of atherosclerotic plaque, composition (calcified, noncalcified, or mixed), and degree of stenosis.
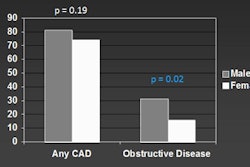
The results showed a few more patients with significant coronary artery stenosis in the cocaine group (n = 17, 25%) versus the control group (n = 14, 21%), a finding that was not statistically significant.
There were no significant differences in stenosed vessels, calcified plaque, or noncalcified plaque; however, cocaine users had significantly more plaque of mixed composition compared to the matched controls (p < 0.05).
 |
| Results show a significant difference (p < 0.05) in the prevalence of mixed plaque composition in the coronary arteries of cocaine users, but no significant differences in the prevalence of calcified or noncalcified plaque, or in the prevalence of significant stenosis. |
"What's known from other studies is that mixed plaque is associated with ACS, and this could be the link, so in our opinion the association might explain the higher prevalence of ACS in those patients with regular cocaine abuse," Ebersberger said.
The association may also be explained in terms of the mechanical properties of mixed plaque, which may be predisposed to rupture during cocaine-induced vasospasm, he said. However, larger studies, as well as basic research to assess the coherence of cocaine and mixed-plaque formations, are needed, Ebersberger said.
When asked after the presentation if patients might tend to underreport cocaine use for the medical record, Ebersberger said that if there is underreporting, it would serve only to strengthen the study's reported association between cocaine use and mixed-plaque atherosclerosis.
The study didn't analyze outcomes, but it did show significant differences between the groups in plaque volumes, Ebersberger said.
The most important data missing from the study is from ACS patients who were triaged to the cath lab. This study was limited to chest pain patients who weren't ultimately referred, he said.