Low-kV dual-energy CT (DECT) of the abdomen is gaining currency as a CT technique that can reveal pathology hidden on traditional imaging techniques, using less radiation and less contrast media. It can also be performed using a variety of methods, each with its own strengths and weaknesses.
"One can potentially use the low-kV image -- even when enhancement is subtle -- for detecting either early disease or residual disease activity that might benefit our clinical colleagues for decision-making," said Dr. Dushyant Sahani, director of CT imaging and associate professor of radiology at Massachusetts General Hospital and Harvard Medical School. "One of the benefits [of low-kV imaging] is that you can process data in a variety of different ways and eventually exploit them in the realm of better diagnosis or improved care for a variety of indications.
Dual-energy CT takes advantage of the different x-ray attenuation properties achieved at different tube energies to differentiate materials such as water, iodine, and fat, Sahani explained in a June presentation at the 2011 International Society for Computed Tomography (ISCT) meeting in San Francisco.
Given a couple of base materials to work with -- for example, water and iodine -- simple calculations can be used to determine how much of each material would be needed to produce the observed kVp measurements. In this manner, the images accurately depict via attenuation how much of each material the scanned anatomy contains.
Virtual monochromatic spectral images can also be generated from these material density images, he said, improving contrast and image quality as well as contrast-to-noise ratio, while reducing beam-hardening artifacts.
 |
| Hepatocellular carcinoma lesions enhance only faintly at 140 kV, but as kV drops the lesions can be seen with increasing confidence. These low-kV images can be produced while keeping the 120-kV image for comparison purposes. All images courtesy of Dr. Dushyant Sahani. |
Among their strengths, low-kV scans are "especially popular for vascular imaging because one can exploit the k edge of iodine to gain more attenuation and, therefore, better image quality," Sahani said.
 |
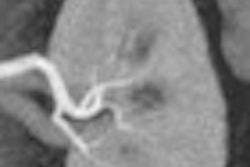
| Low-kV imaging improves vascular imaging. Top, middle rows: Endoleak detection is easier on lower-kV images. The CT angiography study was acquired with only 40 mL of IV contrast. Bottom, on delayed-phase acquisition, 50-keV material composition (MC) image provides enhancement and attenuation values similar to arterial-phase imaging. |
Available techniques for using low-kV imaging run from simple to complex -- the easiest is simply reducing the tube current, he said. Several publications in recent years have shown that simply switching from 140 kV to 100 kV not only improves quality but also reduces radiation dose.
Single- versus dual-source DECT
Sahani's group has been using a lot of low-kV imaging lately, he noted. It can be performed in a single pass using a dual-source CT scanner (Somatom Definition, Siemens Healthcare) or a single-source CT scanner armed with fast kV switching (Gemstone Spectral Imaging mode, GE Healthcare); both of which are used in his facility, Sahani said.
Single- and dual-source DECT have different requirements and different strengths and weaknesses, Sahani said. But while the approach and the algorithms they use are different, the techniques yield similar results. For example, dual-source can perform three-material decomposition (soft tissue, fat, and iodine, for example) versus two-material decomposition (water, iodine) using the single-source DECT scanner.
 |
| Low-kV imaging with single- and dual-source scanners produces similar benefits, though each method has its strengths and weaknesses. |
Single-source DECT can be used for a technique called effective-z imaging, which distinguishes image components based on their atomic number and has been shown to characterize non-uric acid kidney stones. Single-source DECT has advantages over single-energy CT and promises to overcome certain limitations, particularly the following challenges associated with regular CT, according to Sahani:
- Difficulty of tissue characterization
- Limitations in lesion detection (small lesions)
- Image noise and quality issues at low-kV scanning
- Complex scanning protocols (multiphase imaging)
- Higher radiation doses
Both single- and dual-source dual-energy CT can produce monochromatic images, which are the best way to exploit the contrast differences in low-kV images at postprocessing. Monochromatic images generally outperform a scanner's default polychromatic images for subtle contrast enhancement and improved attenuation, Sahani said.
Polychromatic versus monochromatic CT imaging
Polychromatic refers to any normal full-spectrum x-ray beam on the CT scanner, Sahani explained in an interview this month with AuntMinnie.com. "When we say 140 kV, we are referring to the upper limit of the energy spectrum ... but there are other energies in between the upper and lower limits, and a lot of these low energies contribute to peak noise and cause some artifacts," he said. Monochromatic beam generation, on the other hand, is a synthetic process that separates the energies mathematically and eliminates some of them, resulting in generally better-quality images.
A challenge with the use of a polychromatic beam together with single-energy DECT is the generation of beam-hardening artifacts. These artifacts are reduced with the use of monochromatic energies using single-source CT, Sahani said. Still, polychromatic image protocols are more complex.
"One has to get a multiphasic exam, and certainly it leads to limitations in detection and characterization, and, based on the technique, it can also add to the radiation dose," he said. As a result, monochromatic imaging generally produces better results with single-source DECT. "When you move to the monochromatic x-ray, the monochromatic beam satisfies the photon x-ray from the monochromatic x-ray source, and this leads to some of the benefits of monochromatic imaging, including reduced beam-hardening artifact and enhanced attenuation," he noted.
Monochromatic images also improve the detection of iodine-containing substances on low-keV images, he said, leading to improved detection, characterization, and pathology; better evaluation of vascular structures; and reduced iodinated contrast doses.
Through complex mathematics, Gemstone Spectral Imaging is capable of virtually creating a monochromatic image with a range of 40 keV to 140 keV, delivering single-source polychromatic images with reduced artifact. "Gemstone allows you to do that by collecting data at two energies, and it's able to separate the two without much crossover from one to the other," he said. Single-source scanners without its capabilities require two scans to acquire dual-energy CT images.
Blood more visible with low kV
Iodinated contrast is more conspicuous using low-kV imaging. "One can use less contrast volume," Sahani said. "More importantly, we can use low-kV images to make our protocols simpler."
The group has traditionally used a three-phase protocol for vascular imaging, but supported by low-kV imaging it's being abandoned in favor of a two-phase protocol that eliminates the unenhanced phase, he said.
The use of so-called "virtual unenhanced images" created from a single late-arterial-phase acquisition may simplify the protocol even further. Moreover, "in select patients we are validating if we can do a late-arterial-phase scan to exploit monochromatic imaging and generate virtual arterial-phase images," he said. "We are exploring that and validating a single-phase acquisition." The experimental protocol delays scanning for only about a minute after contrast injection, and it uses 50 kV to generate the images.
 |
| Top row: In liver perfusion abnormality, differential enhancement is better seen on material differentiation (MD) iodine image. Bottom row: In CT enterography, MD iodine and lower keV material composition (MC) images accentuate bowel wall enhancement. |
In the imaging of renal cell carcinoma at 120 kV versus 50 kV, lesion enhancement is maximized at the lower kV setting, he said. In a patient with liver metastases, moving from 70 kV to 50 kV improves tumor definition and also better defines the area around the tumor.
"This can translate into a better tumor target for purposes of treatment planning," Sahani said. "For example, in proton therapy for liver tumors they need to have a better definition of the tumor target, and one can exploit this for therapy planning."
 |
| Low-kV imaging improves contrast enhancement, revealing in the case above a renal cell carcinoma at 50 kV that was poorly visualized at 70 kV. |
Processing dual-energy data from virtual monochromatic images fundamentally improves the textual structure of the images, he said, revealing features that would otherwise be invisible, though the appearance is slightly unusual, recalling the appearance of some iterative reconstruction techniques.
In general, the group has found that 50 kV is optimal for vascular imaging, and 70 kV strikes a nice balance for a combination of vascular and solid visceral imaging, producing good image quality, Sahani said.
Low-kV imaging capabilities are promising for improved detection and characterization, better evaluation of vascular structures, and reducing contrast media dose, Sahani concluded. "However, we need to do more work to validate some of these techniques," he said.