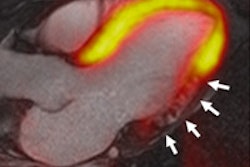
A new comparative effectiveness study has found that 320-detector-row coronary CT angiography (CCTA) is better than SPECT myocardial perfusion imaging (MPI) for diagnosing coronary artery disease (CAD). But MPI still helps avoid unnecessary cardiac catheterization and revascularization.
Radiologists have long suspected that anatomic-based CCTA is more sensitive than functional MPI for CAD diagnosis. That hypothesis was the subject of the Coronary Artery Evaluation Using 320-Row Multidetector CT Angiography (CORE 320) study, which evaluated the diagnostic performance of the two modalities.
CORE 320 was sponsored by Toshiba Medical Systems, the manufacturer of the 320-detector-row Aquilion One CT scanner. Results of the study were presented at the American College of Cardiology (ACC) meeting earlier this month in San Francisco.
The trial involved a cohort of 381 patients with known or suspected coronary artery disease who were examined at 16 facilities in eight countries. Comparative effectiveness data were collected in less than a 10-day period in 2012 as each patient underwent CCTA and SPECT MPI. Quantitative coronary angiography served as a gold standard.
"The strength of this effort is that it is a multicenter trial that had independent core labs and quality assurance for each modality," said principal investigator Dr. Marcelo Di Carli, chief of nuclear medicine at Brigham and Women's Hospital.
The findings show that 320-detector-row CCTA is more sensitive to obstructive coronary artery disease than SPECT MPI, probably making it a better choice for initial CAD diagnosis, Di Carli said. However, SPECT appears to play a mitigating role in ensuring that only flow-limiting lesions are recommended for intervention.
All patients underwent CCTA on the Aquilion One scanner. The protocol included administration of oral or intravenous beta-blockers to slow heart rate, and IV iodinated contrast to acquire 0.5-mm slices of the heart and surrounding tissue for reconstruction and interpretation at a core lab.
Pretrial phantom tests were performed on various types of SPECT platforms to ensure consistent site-to-site performance. Studies were enhanced with technetium-99m (Tc-99m) sestamibi or tetrofosmin. Rest-stress SPECT was performed, with either exercise or pharmacological stresses applied.
Coronary angiography was performed using standard techniques within 60 days after CCTA. Coronary tree segmentation was conducted similar to the CCTA protocol. Quantitative coronary angiography was performed on all vessels with diameters of at least 1.5 mm and 30% stenosed segments.
Higher sensitivity for CCTA
Data analysis based on receiver operator characteristics (ROC) demonstrated CCTA's higher sensitivity and equivalent specificity between CCTA and SPECT MPI on per-patient and per-vessel bases, as well as for 50% and 70% thresholds for diagnostically significant disease. The study also provided insights into the relative performance of the two modalities by patient gender and body mass.
On a per-patient basis for segments with 50% or greater stenosis, the area under the curve (AUC) for ROC was 0.89 for CT and 0.69 for SPECT. On a per-patient basis for segments with 70% or greater stenosis, AUC was 0.86 for CT and 0.74 for SPECT.
CT had higher accuracy rates than SPECT for both men and women, as well as for patients with high body mass (BMI ≥ 30 kg/m2). All differences were statistically significant (p < 0.0001).
On a per-vessel basis for segments with 50% or greater stenosis, AUC was 0.79 for CT and 0.66 for SPECT. In segments with 70% or greater stenosis, AUC was 0.75 for CT and 0.72 for SPECT. All differences were highly significant (p < 0.0001).
An evaluation of efficacy (below) reveals that CCTA's relatively better diagnostic capability stemmed from its higher sensitivity to coronary occlusions. Di Carli and colleagues found essentially no difference in the specificity of the two tests.
| Efficacy of 320-slice CCTA and SPECT MPI CAD detection | |||||
| Sensitivity | Specificity | Positive predictive value | Negative predictive value | ||
| Per patient -- 50% stenosis | |||||
| CCTA | 91% | 74% | 83% | 85% | |
| SPECT | 62% | 67% | 73% | 55% | |
| Per patient -- 70% stenosis | |||||
| CCTA | 94% | 60% | 55% | 92% | |
| SPECT | 71% | 67% | 73% | 73% | |
Coronary CTA and SPECT MPI demonstrated an equal ability to identify high-risk patients with volatile left main stenosis or three-vessel coronary disease, Di Carli said. Based on evaluations of 105 high-risk patients, ROC analysis revealed no significant difference between the 0.79 AUC value for CCTA and the 0.75 AUC values for SPECT.
Effect on revascularization
The CORE 320 study shows that CCTA findings more closely predict whether a patient ultimately undergoes revascularization than results generated with SPECT MPI. The trend, however, may not be a positive one for CT considering the two modalities diagnose high-risk cases equally well.
"The findings suggest that physicians were somehow using the degree of stenosis of CT more frequently than the pattern of ischemia on SPECT to recommend cardiac catheterization," he said.
Further analysis showed that 40% of patients who were revascularized did not have evidence of ischemia on SPECT MPI. Outcomes data were not collected to determine the clinical value or appropriateness of revascularization, Di Carli noted.
The study's limitations include its exclusive reliance on invasive coronary angiography as a gold standard. A functional gold standard, such as fractional flow reserve, would have been beneficial, Di Carli said.
Study disclosure
The CORE 320 study was funded by Toshiba, whose equipment was tested in the trial.