CHICAGO - Coronary CT angiography (CCTA) is vastly underutilized compared to SPECT myocardial perfusion imaging (MPI) in patients with suspected coronary artery disease, despite their status as competitive tests, according to a study presented on Sunday at the RSNA meeting.
In recent years, the discrepancy has been widening, said researchers from Thomas Jefferson University (TJU).
The group found that MPI is used 52 times more frequently than CCTA, owing to a variety of factors that have nothing to do with the suitability of either exam. Use of both tests has been declining in recent years, but CCTA use has fallen far more rapidly, mostly due to reimbursement and, as one might suspect, specialty turf.
"You can debate what should be the appropriate ratio of the use of MPI to CCTA -- maybe that ratio should be 1:1, maybe it should be 5:1, but it certainly shouldn't be as high as 52:1," said Dr. David C. Levin from TJU's Center for Research on Utilization of Imaging Services. "That really is an excessive ratio and it indicates CCTA is greatly underutilized relative to MPI" for diagnosing coronary artery disease.
Both are valuable tests -- in some ways complementary and in other ways competitive -- and there is debate about which test should be used first in patients with suspected coronary artery disease, Levin said.
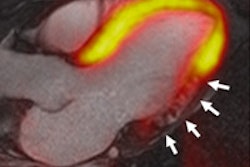
"But evidence has shown that if a patient has a negative MPI, the patient might still have coronary artery disease, even severe coronary artery disease," he said. "But if a patient has a negative CCTA, that patient almost certainly does not have coronary artery disease: that is, the negative predictive value of CCTA is almost 100%."
Levin, along with his Thomas Jefferson colleagues Dr. Vijay Rao, Andrea Frangos, and Laurence Parker, PhD, aimed to compare utilization rates and recent trends between the two imaging procedures.
The data were gathered from the Medicare Physician/Supplier Procedure Summary Master Files for 2000 through 2010, the latest year available. Levin and colleagues used CPT-4 codes for MPI for all 10 years, but they chose CCTA data only for 2006-2010 because in 2006 certain CCTA codes became available, he said.
For each CPT-4 code, data were provided on volume, provider specialty, exam location, and reimbursement. In addition, medical specialty codes identified radiologists and cardiologists as the service provider. The researchers calculated utilization rates per 100,000 Medicare beneficiaries, and Levin and colleagues also looked at trends in CCTA and MPI utilization rates.
The results showed declining use of both exams in recent years but far higher overall utilization of MPI, Levin said. The Medicare MPI utilization rate per 100,000 patients rose from 5,691 in 2000 to 8,573 in 2006 (compound annual growth rate [CAGR]: 7.4%) before it began declining steadily each year thereafter, down to about 7,500 in 2010, for a total CAGR of -3.8% between 2006 and 2010.
 |
| Image courtesy of Dr. David C. Levin. |
For coronary CTA, there was a rapid increase in total CCTA utilization from 99 per 100,000 in 2006 to 210 per 100,000 in 2007.
"Then a surprising thing happened," Levin said. "Here we have a new and useful procedure, and typically when something like that is developed, we see utilization trends continuing to escalate for years. But [instead] we saw utilization trail off progressively over the ensuing years."
Between 2007 and 2010, CCTA utilization began a steady decline, reaching 144 in 2010, he said, and nearly all growth in the modality was due to cardiologists' adoption. By specialty, CCTA rates in 2010 were 81 per 100,000 for cardiologists, 53 per 100,000 for radiologists, and 10 per 100,000 for other specialties.
The ratio of MPI use to that of CCTA was 52:1 in 2010, he said. Why?
For one thing, "MPI is more attractive to cardiologists, who have purchased nuclear cameras for their offices," Levin said. "Reimbursement for CCTA is relatively unfavorable, considering that it's a relatively labor-intensive procedure, there are frequent denials from insurance carriers, and physicians have become discouraged from ordering CCTAs because of the requirements for preauthorization. And then there is the [concern about radiation dose], even though we know that MPI procedures produce about as much as or even more exposure."
As a result, CCTA utilization, despite robust evidence supporting its use, has been decreasing in recent years, as has MPI utilization, he said. Though the appropriate ratio of MPI to CCTA can be debated, it should probably be somewhere between 1:1 and 5:1, not 52:1 -- evidence that the exam is vastly underutilized.
"There appear to be several reasons for this -- all of them bad," Levin said.
Asked after the presentation if he had evidence that utilization in the Medicare population was the same as that of the fiftysomething population more likely to undergo cardiac imaging, Levin said he did not have evidence, adding, "my sense is that it is similar."