Yielding high sensitivity and accuracy, an advanced visualization technique that automatically subtracts bone data from 320-detector-row CT angiography (CTA) scans could substitute for 3D digital subtraction angiography (DSA) in detecting cerebral aneurysms, according to research published online in Radiology.
In a study involving 198 patients with 239 cerebral aneurysms, researchers from the Third Affiliated Hospital of Suzhou University in China found that subtracted volumetric CTA yielded 99.2% sensitivity, 100% specificity, and 99.4% accuracy on a per-aneurysm basis, compared with the current gold standard of 3D rotational DSA.
"Subtracted volumetric CT angiography could replace invasive digital subtraction angiography as the first-line imaging technique for noninvasive evaluation of suspected cerebral aneurysms because of its high diagnostic sensitivity," wrote the research team led by Dr. Wenhua Chen.
Bone-free visualization
While 3D DSA is the gold standard for detecting cerebral aneurysms, it comes with the drawbacks of being invasive, time-consuming, technically demanding, and relatively expensive, in addition to a 0.12% rate of permanent neurologic complication, according to the researchers (Radiology, September 5, 2013).
As a result, the group sought to determine if subtracted 320-detector-row volumetric CTA, which offers bone-free visualization of aneurysms, could accurately detect cerebral aneurysms.
The researchers enrolled 315 patients suspected of having cerebral aneurysm who were scheduled to receive DSA as well as comparative CTA. After 33 patients were excluded for rapid clinical deterioration or having undergone prior surgical clipping or endovascular repair, the final study population included 282 patients (138 men and 144 women with a mean age of 58 years).
Of these patients, 179 (63.5%) had subarachnoid hemorrhage; 31 (11%) had subarachnoid and intraventricular hemorrhage; 15 (5.3%) had subarachnoid and intraparenchymal hemorrhage; 10 (3.6%) had intraparenchymal hemorrhage; 15 (5.3%) had subarachnoid, intraventricular, and intraparenchymal hemorrhage; and 32 (11.3%) had indications such as headache, oculomotor paralysis, tumor, and hydrocephalus, the authors wrote.
All patients received volumetric CTA on an Aquilion One 320-detector-row volumetric CT scanner (Toshiba Medical Systems) using a standardized protocol. After a mask image for subtraction was obtained with a nonenhanced CT protocol, a CTA exam was performed using an intravenous injection of Ultravist contrast (Bayer Schering Pharma).
The subtracted CTA volumetric data were gathered by subtracting the mask image volumetric data from the conventional nonsubtracted CTA volumetric data using the console's software. Bone-tissue data were automatically removed, and the resulting data were reviewed on a Voxar workstation (Toshiba) for 3D visualization using direct volume-rendering techniques or maximum-intensity projections.
The invasive selective angiography exams were performed via the transfemoral approach using an Artis zee biplane DSA unit (Siemens Healthcare). All patients received Omnipaque nonionic contrast material (GE Healthcare). A single 3D DSA acquisition was obtained prior to removal of the catheter from each vessel.
Experienced readers
The volumetric CTA and 3D DSA images were read independently by five neuroradiologists, three of whom had 13 years of CT vascular imaging and angiography experience. The other two observers had 10 such years of experience.
Two of the readers evaluated the subtracted volumetric CTA images, while two evaluated the nonsubtracted volumetric CTA images.
For the purposes of the study, 3D DSA was used as the reference standard. Of the 282 patients, 198 (70.2%) had at least one cerebral aneurysm and there were 239 cerebral aneurysms overall.
| Performance in evaluating cerebral aneurysms | |||
| Sensitivity | Specificity | Accuracy | |
| Nonsubtracted volumetric CTA | 96.7% | 100% | 97.5% |
| Subtracted volumetric CTA | 99.2% | 100% | 99.4% |
"The accuracy of nonsubtracted volumetric CT angiography was lower than that for subtracted volumetric CT angiography, especially for aneurysms adjacent to bone tissue," the authors wrote.
No difference in accuracy
Subtracted volumetric CTA did not differ significantly from 3D DSA in terms of accuracy (p = 0.5). However, nonsubtracted volumetric CTA was significantly less sensitive than both 3D DSA and subtracted volumetric CTA (p = 0.031 and 0.008, respectively).
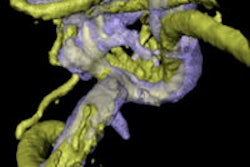
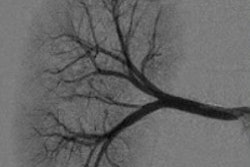
 Volume-rendered image (above) and maximum-intensity-projection image (below) from a 47-year-old woman with a left internal carotid aneurysm (arrows). Images courtesy of Radiology.
Volume-rendered image (above) and maximum-intensity-projection image (below) from a 47-year-old woman with a left internal carotid aneurysm (arrows). Images courtesy of Radiology.

Nonsubtracted volumetric CTA had a comparable diagnostic ability to subtracted volumetric CTA and 3D DSA for detecting aneurysms of the anterior communicating artery, the posterior communicating artery, the anterior cerebral artery, and the middle cerebral artery, the researchers found.
"The aneurysms missed at nonsubtracted volumetric CT angiography were generally located in the internal carotid artery," they wrote. "Detection of cerebral aneurysms adjacent to bone tissue was still challenging at nonsubtracted volumetric CT angiography because of the presence of overlying bone structures."
Subtracted volumetric CTA also had its limitations: The two missed cerebral aneurysms on subtracted volumetric CTA were microaneurysms, which the technique generally struggled to identify. The technique also does not display atherosclerotic plaque and aneurysmal calcification, and it could not present the relationship of aneurysms to bone structures, according to the group.
Nonetheless, the institution has been using 320-detector-row volumetric CTA as its first-line imaging modality to screen patients presenting with subarachnoid hemorrhage possibly caused by ruptured aneurysm, the authors reported.
"Compared with DSA, volumetric CT angiography is simpler and quicker to organize and perform," the authors wrote. "In the emergency setting, volumetric CT angiography can be performed immediately after a diagnosis of subarachnoid hemorrhage on the basis of a routine brain CT scan. Confused, agitated, or uncooperative patients need no more than a short-acting sedative for the performance of volumetric CT angiography, and general anesthesia, which is often required during an emergency DSA workup, can be avoided in most cases."