Both total aortic calcium load and calcium density measured by MDCT are associated with increased mortality risk, according to a new study in the September 23 issue of the Journal of the American College of Cardiology.
The multicenter study of more than 700 patients found that the precise calcium and calcium density measurements associated with risk were different in men and women. However, beyond risk threshold differences between genders, the prognostic value of the scoring system worked the same way in men and women.
"If you look at everything -- age, the severity of aortic stenosis, and all of the factors that can influence survival -- the amount of calcium on the aortic valve has a very strong influence on survival," said co-author Dr. Maurice Enriquez-Sarano, a cardiologist from the Mayo Clinic in Rochester, MN. "If you have more calcium, you will have more mortality after diagnosis" of aortic stenosis.
Moreover, measuring the aortic valve calcium load with MDCT offers significant prognostic value for survival "beyond that obtained from clinical and Doppler echocardiographic data," wrote lead author Marie-Annick Clavel, PhD, along with Enriquez-Sarano and others from the Mayo Clinic, Bichat Hospital in Paris, and Laval University Quebec (JACC, September 23, 2014, Vol. 64:12, pp. 1202-1213).
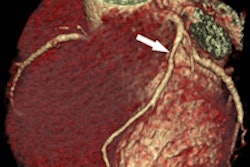
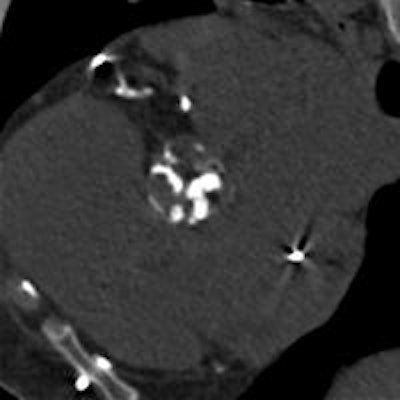
 Aortic valve calcification is easily discernible at MDCT in a patient with extensive calcifications. Image courtesy of Dr. Maurice Enriquez-Sarano.
Aortic valve calcification is easily discernible at MDCT in a patient with extensive calcifications. Image courtesy of Dr. Maurice Enriquez-Sarano.Common condition
Calcific aortic stenosis is a common condition for which aortic valve implantation (AVI) is the only effective treatment. But AVI isn't for everyone, and caution is due for elderly patients in particular. The recent tendency to consider aortic stenosis as a degenerative disease is in line with practice as doctors decide what to do with patients depending on the degree of stenosis.
Previous screening studies using electron-beam CT and a small meta-analysis of data suggest that qualitative assessment of aortic valve calcium (AVC) may be important for prognosis, and there is considerable interest in finding out if this is true in order to help triage patients for invasive or conservative management. This is especially relevant considering that MDCT has been shown to measure aortic calcification accurately.
Because quantification of aortic valve calcium has at least a nonlinear association with hemodynamic data, a somewhat clearer understanding of aortic calcification load and risk has taken form in recent years. But the impact of MDCT-measured AVC load following a diagnosis of aortic stenosis on survival remains unclear despite several echocardiography studies that initially seemed promising, the authors wrote. A pilot CT study suggested that AVC load may be linked to cardiovascular events, but the thresholds were inconsistent and not differentiated by gender.
"We had pilot data showing that measurement of aortic valve calcification with electron-beam CT is reliable ... but the real reason for looking at calcification of the aortic valve is that it is the main cause of aortic stenosis -- whereas calcification of the coronaries is usually just a 'bystander' and not the real obstruction," Enriquez-Sarano said.
MDCT after echo
The researchers sought to evaluate the impact of aortic valve calcium load, both absolute and relative to the size of the aortic annulus (AVCdensity), on overall mortality in patients diagnosed with aortic stenosis under conservative treatment (no valve implantation) and under any treatment approach.
Study teams at three academic centers examined a total of 794 patients (mean age, 73 ± 12 years; 274 women) who had been diagnosed on Doppler echocardiography and on MDCT within the same three-month episode of care. All patients had at least mild aortic stenosis (defined on echo as mean gradient ≥ 15 mm Hg, peak aortic jet velocity ≥ 2.0 m/sec, or aortic valve area ≤ 2 cm2).
The researchers performed noncontrast CT using multidetector scanners from Siemens Healthcare (Somatom Sensation) or Philips Healthcare (Mx8000 IDT 16). Aortic valve calcium measurements were performed on an offline workstation using HeartBeat CS (Philips) or Aquarius iNtuition (TeraRecon). Results were calculated using the Agatston calcium scoring method, with results expressed in arbitrary units (AU).
Based on previous echocardiography research by the authors, aortic valve calcium values of at least 1,274 AU in women and 2,065 AU in men were set as the optimal cutoff for defining severe AVC. To account for variability in body size, a second measure indexing AVC to the cross-sectional area of the aortic annulus was used, with AVCdensity thresholds of 292 AU/cm2 for women and 476 AU/cm2 for men.
Coronary calcifications, visible in the CT scans and also measured, were considered severe when they were greater than the median value in the patient population, the authors noted. Echocardiography and CT were performed within nine days of each other. The primary study end point was overall survival under medical treatment, while secondary end points included cardiovascular death under medical management and survival during the entire follow-up period, regardless of AVI status.
Risk from severe calcifications
During follow-up of 3.1 ± 2.6 years, there were 440 total aortic valve implantations and 194 deaths, including 115 under medical treatment. Univariate analysis showed a strong association of both absolute AVC and AVCdensity with survival (p < 0.0001 for both), Clavel and colleagues reported.
After adjusting for a wide range of factors, including age, sex, coronary artery disease, diabetes, patient symptoms, hemodynamic assessment of aortic stenosis severity, and left ventricular ejection fraction, both severe absolute AVC and severe AVCdensity independently predicted mortality under medical treatment.
The overall five-year survival after diagnosis of aortic stenosis for the entire cohort was 65% ± 3% under medical management and 68% ± 2% under any care -- that is, medical and/or surgical management.
"That's a very important finding, and the first time calcium measured by CT is proven to affect long-term survival after diagnosis of aortic stenosis," Enriquez-Sarano said.
Unlike the total calcium score, the calcium density score accounts for different patient sizes, and higher density negatively affects survival -- based on 300 AU/cm2 in women and 475 AU/cm2 in men (both p > 0.24). Men have "big hearts that have bigger aortic valves and more calcium, so you have to take into account aortic annulus size" and combine the calcium score and the calcium density score to get the best prognostic information in terms of mortality, he said.
Severe absolute AVC and severe AVCdensity also independently predicted overall mortality, even when the researchers adjusted for time-dependent AVI.
The link between calcium load and mortality is "incremental in all clinical and Doppler echocardiographic measures ... and persists in patients with hemodynamically severe aortic stenosis," the authors wrote.
CT as the referee when Doppler is unclear
Because quantification of the calcium load is strongly but not linearly associated with hemodynamic measures of aortic stenosis severity, MDCT adds incremental value to Doppler echocardiography, and it can serve as a tiebreaker on the need for intervention when Doppler results show a discordant gradient, Enriquez-Sarano noted.
Now that physicians have CT to aid decision-making, treatment choices will be much better informed and patient care will be improved, he said.
In any case, the simple, low-dose, noncontrast coronary calcium CT scan is done in diastole at 70% to 75% of the cardiac cycle, and the score is calculated by software. There's every reason to use it routinely, he added.
Going forward, the team plans to analyze how CT results influence outcomes and heart failure in various subsets of patients, and then extend the scans into the various centers so they can be applied and eventually incorporated into societal guidelines.