Combined dual-energy coronary CT angiography and CT myocardial perfusion imaging (CCTA-MPI) improves both the identification and discrimination of ischemia-causing coronary artery stenoses over CCTA alone, according to a Korean study presented at last week's RSNA meeting.
Assessed in a sizable cohort of nearly 200 patients with significant stenoses at CCTA, the combined scans significantly improved the characterization of flow-limiting disease.
Compared with combined invasive coronary angiography/cardiac MR-MPI, CCTA with stress dual-energy CT (DECT) and MPI improves the predictive value of ischemia-causing coronary artery stenoses versus CCTA, but it only mildly improves the diagnostic performance of stress DECT-MPI alone, concluded Dr. Sung Min Ko, from Konkuk University Hospital in Seoul, South Korea, and colleagues.
 Dr. Sung Min Ko from Konkuk University Hospital.
Dr. Sung Min Ko from Konkuk University Hospital.The researchers previously showed that DECT-MPI is feasible and provides good diagnostic accuracy for significant coronary artery disease, and that added to CCTA it can provide incremental diagnostic value in the detection of significant disease, Ko said.
"But to date, large-scale studies with comparisons against a combined end point of both myocardial perfusion defects and anatomically obstructive coronary stenosis are lacking," he said.
The current study aimed to determine the diagnostic performance of stress DECT-MPI for identifying and excluding coronary artery stenoses that cause ischemia. The researchers prospectively examined 192 consecutive patients who underwent CCTA, DECT-MPI, invasive coronary angiography, and cardiac MR with MPI (CMR-MPI).
They used both DECT-MPI and CMR-MPI to look for the presence or absence of myocardial perfusion defects, while CCTA and invasive coronary angiography images were examined for the presence or absence of anatomically obstructive stenosis, defined as a stenosis greater than 50%.
The primary end point was lesion-specific ischemia on a per-patient basis, as defined by a combination of greater than 50% stenosis at invasive coronary angiography and an associated perfusion defect at CMR-MPI. In exploratory analyses, DECT-MPI and CCTA were compared directly with CMR-MPI and invasive coronary angiography, respectively.
Among the 192 patients examined, (135 men, 57 women; mean age, 63.1 ± 8.0 years), 144 (75%) patients and 257 (45%) vascular territories showed ischemia-causing coronary stenoses.
Using electrocardiogram gating, the study team scanned the patients with a dual-source scanner (Siemens Healthcare) at 60% to 75% of the RR interval (140 kV and 100 mAs for the A tube; 80 kV and 165 mAs for the B tube). Scans began four minutes after adenosine infusion and followed injection of iodinated contrast using bolus tracking, Ko said.
Two radiologists independently evaluated the images based on a modified 17-segment American Heart Association model. The average heart rate was 57 beats per minute (bpm) ± 12 for CCTA and 74 bpm ± 16 for DECT-MPI.
On a per-vessel basis, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for detecting ischemia-causing coronary lesions favored the combined exam, the researchers found.
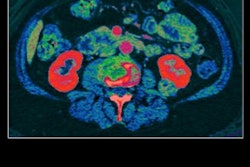
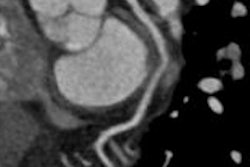
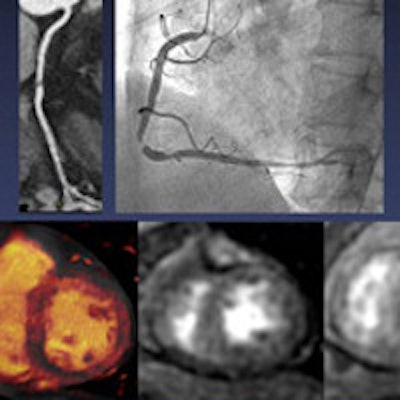
 Left to right: Rest single-energy CT does not show perfusion defect in left ventricular myocardium. Stress DECT shows perfusion defect in midinferoseptal and inferior wall, corresponding to right coronary artery territory. Rest and stress perfusion MRI confirmed the reversible perfusion defect in right coronary artery territory. No myocardial infarction was seen in the left ventricular wall on delayed contrast-enhanced MRI. Image courtesy of Dr. Sung Min Ko.
Left to right: Rest single-energy CT does not show perfusion defect in left ventricular myocardium. Stress DECT shows perfusion defect in midinferoseptal and inferior wall, corresponding to right coronary artery territory. Rest and stress perfusion MRI confirmed the reversible perfusion defect in right coronary artery territory. No myocardial infarction was seen in the left ventricular wall on delayed contrast-enhanced MRI. Image courtesy of Dr. Sung Min Ko.| Detection of ischemia-causing coronary artery stenoses | |||
| DECT-MPI and CCTA | DECT-MPI alone | CCTA alone | |
| Sensitivity | 88% | 91% | 95% |
| Specificity | 82% | 75% | 45% |
| PPV | 79% | 75% | 63% |
| NPV | 89% | 92% | 94% |
The area under the receiver operator characteristics curve for DECT-MPI and CCTA was 0.85, compared with 0.75 for CCTA alone (p = 0.001).
"DECT is a novel method that allows for mapping of myocardial contrast for evaluation of myocardial perfusion," the authors wrote in their study abstract. "Stress DECT-MPI provides clinical benefit to patients with insufficiently evaluated coronary lesions by CCTA alone."