SAN DIEGO - What are the top clinical applications of dual-energy CT (DECT), and in what ways does the technique add value to diagnostic imaging? Radiologists from Stanford and Duke University tackled these and similar questions in a session at the 2018 International Society for Computed Tomography (ISCT) symposium.
Advancements to CT technology have led to the emergence of DECT as a means of enhancing various aspects of image visualization. From improving lesion conspicuity to overcoming uncertainty in characterizing small lesions, DECT offers numerous diagnostic advantages compared with conventional CT, without altering costs, scanning times, or radiation dose, Dr. Bhavik Patel of Stanford told meeting attendees.
"There are multiple areas for which dual-energy CT can help improve clinical practice," added Dr. Daniele Marin of Duke University. "I think the key is going to be able to streamline the workload so that we are able to use this technology without being overwhelmed by the amount of information it can deliver."
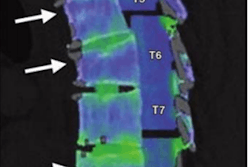
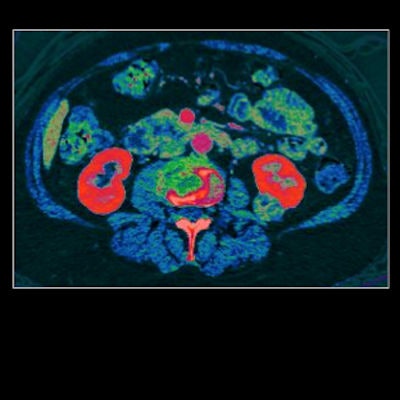
 Abdominal dual-energy CT scan of a patient with renal cell carcinoma (RCC). Image courtesy of Dr. Bhavik Patel.
Abdominal dual-energy CT scan of a patient with renal cell carcinoma (RCC). Image courtesy of Dr. Bhavik Patel.Added value for free
DECT enables clinicians to acquire multiple sets of imaging data at different beam spectra, or energy levels. They can thus view scans at low and high energy levels, depending on which level is best for the case at hand, rather than relying wholly on a single-energy dataset.
What value does this add to diagnostic imaging? Patel pointed to five general categories highlighting the benefit of using DECT instead of standard CT:
-
Improved image quality: Compared with standard CT, DECT is associated with considerably less noise. It is also less susceptible to beam hardening, helping with metal artifact reduction.
In a sample case, a radiologist reviewed a standard chest CT scan of an emergency patient and was unable to rule out aortic injury. Typically, a patient in this scenario would have to undergo yet another exam to clarify the findings. The availability of a low-energy (40-50 keV) DECT dataset for this patient effectively allowed the clinicians to rule out aortic injury without having to repeat the exam.
"The added value here is that we're reducing waste and improving utilization," Patel said.
- Improved lesion detection: Low-energy scans are particularly optimal for the attenuation of iodine contrast. And this improved contrast visualization can facilitate the detection of small, difficult-to-find lesions by increasing their visibility and reducing the pseudoenhancement often seen surrounding kidney and liver lesions.
-
Improved lesion characterization: Furthermore, clinicians can create virtual monochromatic images from the DECT dataset to enhance the visibility of obscure findings that would otherwise prove difficult to characterize on conventional CT. Patel and colleagues came across several instances where a liver tumor could have been either benign or malignant on standard contrast-enhanced CT.
"We used dual-energy CT to help radiologists better and more confidently distinguish and differentiate benign from malignant lesions," he said.
- Reduced overall radiation dose: Some conditions call for multiphasic acquisitions that require two or more CT exams. DECT provides all of the relevant information that these multiphase exams do, but with a single exam.
- Reduced contrast dose: DECT requires a smaller dose of contrast than typical CT angiography exams.
"I think the strategy to improve [diagnostic imaging] with DECT is to leverage the inherent properties of the technology," Patel said. "You don't have to do anything additional to get a lot of this information."
It takes time
 Dr. Bhavik Patel from Stanford University.
Dr. Bhavik Patel from Stanford University.The advantages of using DECT have remained somewhat obscured by several myths surrounding the technique, including that DECT doubles radiation dose, lengthens scanning times, and increases costs, Patel noted. These misconceptions may have contributed to the slow uptake of DECT in previous years.
Clinical experience has shown that DECT actually requires more or less the same radiation dose and scanning time as standard CT yet offers a higher sensitivity and specificity for diagnosis -- making life easier for the radiologist, he said.
What's more, the large-scale application of DECT can lead to long-term capital gains. Most healthcare institutions perform a mixture of single-phase and multiphase standard CT exams on a daily basis. Using DECT in place of standard CT hospital-wide would lead to fewer total exams performed to manage the same number of patients, as DECT removes the need for multiphase CT exams.
"Dual-energy CT provides several economic advantages from any perspective that you think about, from the clinical practice side, the radiologist side, and, I think, the most important one, the overall patient health side," he said.
So if DECT tops standard CT on so many fundamental fronts, why are clinicians not turning to the advanced modality more often?
Perhaps because changes to clinical protocol take a long time to implement in healthcare, according to Patel. Radiologists could help accelerate this process by making it easier for other physicians to access DECT data. This could entail making sure the data are available in PACS, as well as being strategic about what type of DECT data (low- or high-energy scans) they send to referring physicians.
"We are beginning to see an increasing use of [DECT] in hospitals, and this will continue to grow," he told AuntMinnie.com. "In the future, I think there will be less of a distinction between single-phase CT and dual-energy CT; we will just refer to CT as multienergy CT."