Preoperative CT in patients with periampullary adenocarcinoma should include slices of less than 2.5 mm to decrease the likelihood of an unexpectedly pancreaticoduodenectomy (Whipple procedure).
The results could help clinicians better prepare for surgery for this disease by effectively directing CT imaging protocols, wrote a team led by Christian van der Pol, MD, of McMaster University in Hamilton, Ontario, Canada. The study findings were published March 5 in the American Journal of Roentgenology.
"If curative-intent surgery is planned in patients with periampullary carcinoma, preoperative CT should be performed using reconstructions smaller than 2.5 mm to reduce the likelihood of incorrect staging," the group noted.
Surgeons use the Whipple procedure to treat pancreatic cancer, chronic pancreatitis, or bile duct obstruction, the team explained. But up to 20% of these procedures are unexpectedly terminated due to intraoperative findings, it noted. To investigate what imaging and clinical factors might be associated with this outcome, Van der Pol and colleagues conducted a study that included data from 10 U.S., Canadian, and French institutions; the information came from 360 adults with periampullary adenocarcinoma who underwent Whipple procedures between January 2016 and December 2022.
Of the study cohort, 180 patients experienced unexpected termination of the Whipple procedure, while 180 patients underwent the procedure successfully. The researchers matched patients from each group by sex and categorized them into five-year age blocks and tracked the following measures:
- Cancer type
- Tumor size and resectability on CT
- CT reconstruction slice thickness including by phase
- Number of phases
- Multiplanar imaging
- Reconstruction at the workstation
- Possible metastases reported
- Structured versus unstructured report
- Reporting radiologist's experience
- Hepatic steatosis
- Preoperative liver MRI
- Endoscopic ultrasound
- Endoscopic retrograde cholangiopancreatography
- Multidisciplinary review
- Neoadjuvant therapy and response
- Serum CA 19-9 and CEA levels
Overall, the researchers found that Whipple procedures were most frequently terminated due to metastases (67%) and by locally unresectable disease (28%).
The investigators found two factors were associated with Whipple procedures: preoperative CT that included only slice thicknesses of 2.5 mm (odds ratio [OR], 4.28, with 1 as reference) or more and serum CA 19-9 levels of 37 U/mL or more (OR, 3.75).
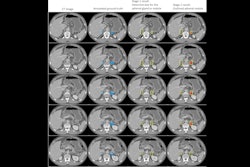
 70-year-old woman with pancreatic ductal adenocarcinoma. Left: Preoperative axial arterial (pancreatic) phase image shows primary tumor in pancreatic head (arrow), which was deemed resectable. Right: More superior axial image in same phase shows dilated main pancreatic duct (arrow). Thinnest CT slices were 1 mm thick. Whipple procedure was completed. Images and caption courtesy of the ARRS.
70-year-old woman with pancreatic ductal adenocarcinoma. Left: Preoperative axial arterial (pancreatic) phase image shows primary tumor in pancreatic head (arrow), which was deemed resectable. Right: More superior axial image in same phase shows dilated main pancreatic duct (arrow). Thinnest CT slices were 1 mm thick. Whipple procedure was completed. Images and caption courtesy of the ARRS.
The study results show promise for improving the success of periampullary adenocarcinoma surgery, according to the authors.
"Multiphase thin-slice CT acquired with slice thicknesses of less than 2.5 mm represents a critical step in the workup of patients with potentially resectable periampullary cancer," they concluded. "Further research and technologic advancements need to be made in this area, and all patient factors must be considered when deciding whether to operate with curative intent."
The complete study can be found here.