Adding dark-field radiography to conventional chest radiography can improve pneumothorax detection, as well as substantially reduce reading times, according to a study published December 18 in Radiology: Cardiothoracic Imaging.
The finding is from a prospective experiment in 100 patients with and without pneumothorax, with dark-field radiography enhancing diagnostic confidence for radiologists without a loss of sensitivity and specificity, noted lead author Florian Gassert, MD, of the Technical University of Munich (TUM) in Germany, and colleagues.
“Dark-field imaging may enhance the detection of pneumothoraces that could be missed with conventional radiographs alone,” the group wrote.
Pneumothorax, or collapsed lung, poses a significant diagnostic challenge in clinical practice, and if left untreated, may rapidly progress to life-threatening respiratory failure, the authors explained. Chest radiography is widely used to detect the condition for its accessibility, low cost, and relatively low radiation dose, yet its sensitivity is limited, especially where signs may be obscured by overlying anatomic structures such as the ribs or heart, they noted.
Conversely, dark-field radiography is an emerging experimental technology that captures ultrasmall-angle x-ray scattering at interfaces between air and tissue in alveoli in the lungs. The technique is based on modifying an existing x‑ray scanner with interferometers and enables the simultaneous acquisition of attenuation and dark-field images. In previous studies, it has shown promise in detecting pulmonary conditions that affect alveolar structure, such as emphysema, fibrosis, and COVID-19 pneumonia.
To further evaluate a prototype they developed, the group at TUM recruited 36 individuals with clinically confirmed pneumothorax and 64 healthy controls. Between March 2022 and September 2023, participants underwent imaging, with attenuation-based and dark-field images acquired.
Five readers with varying levels of experience in clinical radiology and in dark-field imaging assessed the attenuation-only radiographs and then, after a four-week interval, assessed dark-field overlay images. During the second session, readers were able to toggle the overlayed dark-field signal on and off, allowing them to switch between the overlay and the pure attenuation image.
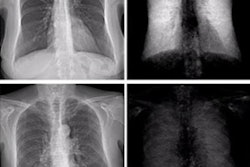
 Examples of attenuation-based conventional radiographs (A-D) without and (E-H) with dark-field overlay in a (A, E) 49-year-old male participant without pneumothorax and (B-D, F-G) three participants with pneumothorax. The participants with pneumothorax included (B, F) a 32-year-old male participant with left-sided apical, pronounced pneumothorax (arrowheads), (C, G) a 72-year-old female participant with a small right-sided apical pneumothorax (arrowheads) in whom thoracic drainage has already been inserted on the right side, and (D, H) a 75-year-old female participant with a small right-sided apical pneumothorax (arrow), in whom the pneumothorax is even more obvious on the radiograph with dark-field overlay (arrowheads). (C, G) In the 72-year-old female participant, the pneumothorax line is hard to recognize on the conventional radiograph without overlay (due to overlay of ribs); it appears to be easier to recognize on the image with the dark-field overlay due to the signal loss in that area. (D, H) In the 75-year-old participant, the small pneumothorax is difficult to recognize on both the image without overlay (D) due to ribs in that area, and the image with dark-field overlay (H) due to an ill-defined margin of the dark-field signal combined with residual beam-hardening-induced dark-field signal from the ribs. In G, the dark-field signal in the lower left corner is due to an attached band-aid.RSNA
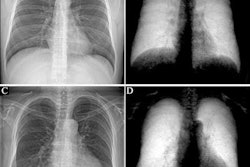
Examples of attenuation-based conventional radiographs (A-D) without and (E-H) with dark-field overlay in a (A, E) 49-year-old male participant without pneumothorax and (B-D, F-G) three participants with pneumothorax. The participants with pneumothorax included (B, F) a 32-year-old male participant with left-sided apical, pronounced pneumothorax (arrowheads), (C, G) a 72-year-old female participant with a small right-sided apical pneumothorax (arrowheads) in whom thoracic drainage has already been inserted on the right side, and (D, H) a 75-year-old female participant with a small right-sided apical pneumothorax (arrow), in whom the pneumothorax is even more obvious on the radiograph with dark-field overlay (arrowheads). (C, G) In the 72-year-old female participant, the pneumothorax line is hard to recognize on the conventional radiograph without overlay (due to overlay of ribs); it appears to be easier to recognize on the image with the dark-field overlay due to the signal loss in that area. (D, H) In the 75-year-old participant, the small pneumothorax is difficult to recognize on both the image without overlay (D) due to ribs in that area, and the image with dark-field overlay (H) due to an ill-defined margin of the dark-field signal combined with residual beam-hardening-induced dark-field signal from the ribs. In G, the dark-field signal in the lower left corner is due to an attached band-aid.RSNA
Dark-field chest radiographs demonstrated clear signal loss in collapsed lung regions of participants with pneumothorax.
Sensitivity for pneumothorax detection was 84.2% with conventional radiography and 87.4% with dark-field chest radiography (p = 0.61).
The addition of dark-field imaging reduced median reading time by 60%, from 30.8 seconds to 10.3 seconds (p < 0.001).
“Dark-field chest radiography substantially reduced reading time without compromising sensitivity for pneumothorax detection compared with conventional radiography in clinical practice,” the group wrote.
Although the improvement in sensitivity with the addition of the dark-field image overlays was modest, the technique’s ability to accelerate the diagnostic process without compromising accuracy supports its potential integration into routine clinical workflows, the group wrote.
Ultimately, the technology is still in the prototype stage and without defined commercial costs and is being developed as a complementary tool for specific indications rather than a replacement for standard attenuation-based images, the researchers added. The results of this study warrant further investigation, they concluded.
The full study is available here.