A time-resolved 3-tesla MR angiography (MRA) technique that uses less contrast dose than conventional high-resolution MRI has some advantages in the abdominal aorta, but its lower signal-to-noise ratio means it probably won't supplant conventional MRA, according to a study in the May Academic Radiology.
Despite that limitation, researchers from the University of Tübingen in Germany and the University of California, Los Angeles concluded that time-resolved abdominal 3-tesla MRA "might be particularly useful in patients with limited breath-hold capabilities or when limiting contrast dose is desirable." The lead author of the study is Dr. Ulrich Kramer from the diagnostic and interventional radiology department at the University of Tübingen (Acad Radiol, May 2010, Vol. 17:3, pp. 564-576).
In the paper, the researchers noted how 3D contrast-enhanced MRA has become a substitute for digital subtraction angiography (DSA), which has been the standard of reference to evaluate abdominal vasculature and major branches. However, one challenge of the technique is the need to time the contrast bolus precisely, such as through the use of a contrast timing run.
Time-resolved MRA is one possible solution, and the technique has been used at 1.5-tesla imaging in the peripheral vasculature, carotid arteries, and pulmonary and aortoiliac arteries. But time-resolved 1.5-tesla MRI hasn't been employed in the abdomen because of the larger volume of coverage required, limited spatial resolution, and reduced signal-to-noise (S/N) ratio caused by parallel acquisition techniques.
Kramer and colleagues sought to determine whether the approximate doubling in S/N ratio for 3-tesla scanners relative to 1.5-tesla systems might make time-resolved 3D 3-tesla MRA appropriate for the abdominal aorta and its major branches.
The group prospectively enrolled 22 consecutive patients (8 men, 14 women; mean age, 43.9 years; range, 19-66) in the study. Patients with contraindications to MRI, such as pacemakers, history of allergic reactions to MR contrast agents, or claustrophobia, were excluded.
Both the time-resolved and high-resolution scans were conducted on a 3-tesla whole-body MRI system (Magnetom Tim Trio, Siemens Healthcare, Erlangen, Germany) equipped with 32 receiver channels and a fast gradient system. A six-element phased-array surface coil was used anteriorly and six elements of the spine matrix coil were used posteriorly to image the vasculature from the proximal abdominal aorta to the inguinal ligaments, including the renal and pelvic arteries.
The 22 patients received time-resolved contrast-enhanced MRA, followed by conventional high-spatial-resolution contrast-enhanced MRA during the same exam without repositioning.
Contrast protocol
Patients were injected with a dose of 3 to 5 mL of gadopentetate dimeglumine (Magnevist, Bayer HealthCare Pharmaceuticals, Leverkusen, Germany) at a rate of 3 mL/sec, followed by a 30-mL saline flush at the same injection rate. Patients also received 0.1 mmol/kg of gadopentetate dimeglumine for single-phase contrast-enhanced MRA.
They were asked to hold their breath for as long as possible during the MR scans, with image acquisition starting after a fixed delay of eight seconds after contrast material injection.
Total examination time of the MRI scans was approximately 25 ± 5 minutes, including patient positioning. In all patients, both time-resolved and conventional 3D contrast-enhanced MRA were performed successfully after uneventful administration of the contrast agent.
MRA findings
With the conventional high-resolution MRA protocol, the researchers found and evaluated 242 arterial segments in 22 patients. In nine of 22 patients (41%), a total of 12 accessory renal arteries were viewed, with nine (75%) of the dozen located on the right side and three (25%) on the left side.
In six patients (27%), renal artery stenosis or fibromuscular dysplasialike lesions were detected. Four patients (18%) were referred to DSA to confirm MRA findings and/or for interventional treatment, such as percutaneous balloon angioplasty or stent placement.
Both readers in the study considered overall image quality and diagnostic performance with high-resolution MRA to be greater than with images from the time-resolved technique. They also both noted improved depiction of the smaller vessel branches relative to vessel conspicuity on a per segment basis with high-resolution versus time-resolved MRA.
In addition, they found "no subjective significant differences with respect to the artifact scoring system between the use of time-resolved and single-phase 3D [contrast-enhanced] MRA in this study," the authors wrote. "Artifacts seen on both sequence types included predominantly motion artifacts."
 |
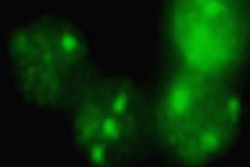
| Six consecutive coronal maximum-intensity projection images from a 3D time-resolved contrast-enhanced MRA of a 43-year-old woman presenting with secondary arterial hypertension. The suprarenal and infrarenal abdominal aorta, as well as the renal arteries (b, white arrows) are clearly delineated. In the venous phase, an insufficiency of the left ovarian vein (e and f, open arrow) was found as a secondary finding. Image courtesy of Academic Radiology. |
'Dynamic information'
Based on the results, the researchers concluded that time-resolved MRA's "addition to a standard abdominal MR protocol can provide useful dynamic information in conditions such as rapid parenchymal and/or venous enhancement, in which high-spatial-resolution contrast-enhanced MRA may lack sufficient temporal resolution."
The technique also "might be valuable because of the acquisition times of less than two seconds per dynamic data acquisition. In contrast, even at higher field strength ... breath-hold times up to 20 seconds are necessary for conventional contrast-enhanced MRA of the entire abdominal aorta, and patients with liver disease or respiratory limitations are often not capable of holding their breath this long."
The authors proposed that the technique not be used as a sole diagnostic tool, but "rather as a supplement to a high-spatial-resolution acquisition. Therefore, it may be used to measure circulation times (e.g., for conventional high-spatial-resolution contrast-enhanced MRA) or to assess contrast material kinetics."
By Wayne Forrest
AuntMinnie.com staff writer
April 19, 2010
Related Reading
CE-MRA helps plan treatment of patients with peripheral artery issues, November 10, 2009
3T MRA best detects small unruptured intracranial aneurysms, November 10, 2009
Quantitative MRA shows promise in stenosis detection, February 12, 2009
MR angiography offers greater detail in vascular imaging, March 10, 2006
High resolution, fast acquisition give 3D MRA edge in abdomen, January 20, 2006
Copyright © 2010 AuntMinnie.com