A computer-aided detection (CAD) algorithm that detects coronary artery stenosis at coronary CT angiography (CTA) not only helped less experienced readers find more lesions, it ruled out adverse cardiac events for more than a year in patients who had disease symptoms but were read by CAD as negative.
In the latter series, CAD actually outperformed the human readers in stenosis detection, said Dr. U. Joseph Schoepf from the Medical University of South Carolina in Charleston.
Schoepf presented the two new studies examining the investigational CAD scheme in May at the International Society for Computed Tomography (ISCT) meeting in San Francisco. Both studies build on the success of the group's initial experience with the algorithm in 59 patients, presented at last November's RSNA meeting. That study showed CAD's high sensitivity (74% per vessel, 100% per patient) and specificity (83% per vessel, 65% per patient) for detecting significant stenosis, but with a number of false positives.
The investigational system (COR Analyzer, Rcadia Medical Imaging, Auburndale, MA) works by first automatically identifying and segmenting large anatomic structures such as the aorta and mediastinum. The next step is identifying the left and right coronary tree ostia. Tracking and segmentation of the coronary tree and extraction of vessel centerlines are then followed by automated labeling of the coronary arteries and automated stenosis detection.
 |
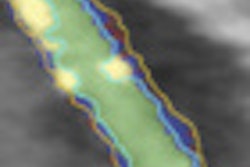
| The investigational CAD algorithm automatically tracks and segments the coronary tree, extracting vessel centerlines and labeling them before performing automated stenosis detection and marking of target vessels. All images courtesy of Dr. Joseph Schoepf. |
CAD's impact on readers
With the initial clinical study under their belts, the researchers moved on to evaluate how the algorithm affected clinicians reading CT angiography exams in a study of 50 patients undergoing coronary CTA.
"We had five readers with different levels of experience: two residents, a fellow, and one cardiologist and a radiologist who were the more experienced readers," Schoepf said.
After an initial read without CAD, the readers re-examined all of the datasets three months later with the aid of CAD. Across the board, detection improved with the use of CAD, he said:
- Inexperienced readers improved from 65% sensitivity per vessel to 82% and from 86% sensitivity per patient to 100%.
- Experienced readers improved slightly from 92% to 96% per vessel but showed no change per patient.
- The false-negative rate dropped from an average of 2 to 0 for inexperienced readers but did not change for the expert readers.
 |
| Receiver operator characteristics (ROC) analysis shows that the area under the curve rose for all readers, but improvement was greater among the less sensitive readers. |
"The more experienced readers really didn't benefit much from the addition of computer-aided detection," Schoepf said. "But if you look at our two residents, their performance was substantially boosted to a whopping 100% negative predictive value when they used the system to aid their interpretation."
On the other hand, one resident's specificity dropped from 78% to 63% when aided by CAD. "He was swayed by false-positive [CAD] detection marks to call a positive finding a significant stenosis when it was not," Schoepf said.
 |
| Above, negative predictive value (NPV) of coronary CTA diagnosis improved for inexperienced readers with the use of CAD, while the effect on specificity (below) was mixed. |
 |
CAD's prognostic powers
Another question central to both researchers and healthcare payors is what happens to patients after the scan -- including how well CAD is able to pick the chest pain patients who can be safely discharged after a negative exam.
To that end, the group looked at 247 triple-rule-out coronary CTA studies in patients presenting with acute chest pain, 209 of whom had no emergent pathology (suspected acute coronary syndrome, pulmonary embolism, or acute aortic syndromes).
There were 131 patients (63%) for whom a CAD detection mark was deployed, and 78 patients for whom no CAD marks were deployed, Schoepf said.
During a mean follow-up period of 12.8 ± 7.0 months, 28 patients with CAD marks had major adverse events, he said. But after one year or more, "none of the patients who were cleared by the system had any major adverse cardiac events" Schoepf said, demonstrating 100% negative predictive value for the CAD system.
 |
| Image shows 64-slice coronary CTA in a 61-year-old woman with body mass index greater than 40kg/m2 and atypical chest pain. CAD detected significant stenosis caused by noncalcified plaque in the proximal right coronary artery confirmed by invasive catheter angiography. The lesion was missed by three of five readers, due to high image noise. |
Considering the clinical scenarios, CAD has many potential uses, including triage of patients in the acute chest pain setting or in peripheral hospitals when no experienced readers are available, he said.
In high-volume hospitals, CAD can help staff members prioritize their efforts on patients who need immediate care, while easing bottlenecks and other workflow issues.
As a second reader, CAD could help increase sensitivity, reduce interpretation time, and "obviously, if you're not that confident yet in your coronary CTA interpretation, CAD may boost your confidence and performance as a second pair of eyes," Schoepf said.
Unfortunately, cardiac CAD is not yet integrated into PACS, the effect on interpretation time is unclear, and specificity could be better. But, overall, the prospects for CAD's improving patient care are extremely positive, he said.
"There's CAD for colonic polyps and lung nodules and many other applications, so I felt there was a big discrepancy that really needed to be addressed -- because if you think about the pathology, it's relatively easy to detect those lesions compared to coronary artery stenosis," Schoepf said, because it's a less complex task for computer systems.
For that matter, the diseases other CAD systems detect "kind of pale in comparison to cardiovascular disease, which has the highest mortality and the greatest socioeconomic importance in the western world," Schoepf said.
By Eric Barnes
AuntMinnie.com staff writer
June 1, 2010
Related Reading
CAD takes on arteries with coronary stenosis detection, November 19, 2009
Automated segmentation could improve fetal heart echo, November 6, 2009
CARS report: Fuzzy theory yields sharper CTA images, June 27, 2008
3D development outpaces facilities' readiness, June 23, 2008
Video game technology speeds beating-heart surgery, June 9, 2008
Copyright © 2010 AuntMinnie.com