In theory, the hybrid offers the best of both worlds, whether it's a redder rose with a sweeter smell or a smaller dog with curlier hair. Hybrid imaging technologies, such as PET/CT devices, combine CT’s anatomic data with PET’s functional images to yield not only quicker CT acquisition times, decreasing the overall scan duration, but a virtually noiseless source of attenuation information that can be used to reconstruct attenuation-corrected PET images.
But hybrids also pose particular challenges, and PET/CT technology is no different, according to an article published in the Journal of Nuclear Medicine by Swiss researchers at the University Hospital of Zurich (JNM, May 2003, Vol.44:5, pp.732-738).
Specifically, Dr. Elena Dizendorf and colleagues studied the errors introduced by oral CT contrast agent in PET emission studies, using phantom measurements and patient data to determine their cause and significance.
CT images produce maps of photon attenuation between 40 to 140 keV; existing dual-modality scanners convert them into attenuation coefficients at 511 keV for PET attenuation correction. Algorithms are then applied that account for different properties of soft tissue and bone, but not necessarily material with other attenuation characteristics, like oral CT contrast agents. When these agents are used, CT-based attenuation correction produces erroneous PET standardized uptake values (SUVs).
The study included 10 patients with gastrointestinal diseases who underwent whole-body PET/CT scans with oral CT contrast agents between February and June 2002. The patients’ mean age was 56 years.
The patients received contrast agent one hour before being scanned. Four received 1,000 mL of Gastrografin, and six received 1,000 mL of Micropaque Scanner. The control group consisted of five men and five women, mean age 63, who were scanned without oral CT contrast agent and who had no gastrointestinal tract tumors.
Forty-five minutes before being scanned, participants received 370 MBq of FDG. All scans were performed on a Discovery LS unit (GE Medical Systems, Waukesha, WI). Dizendorf and her team acquired CT data first before acquiring PET emission data in two-dimensional mode. CT and PET images were reconstructed with a field of view of 500 mm and a 4.25 mm slice thickness. Iterative reconstruction and CT-based attenuation correction were used for the PET SUV images.
The researchers also used a National Electrical Manufacturers Association (NEMA) phantom that consisted of two inserts of Gastrografin and Micropaque Scanner in a main cylinder filled with water. The phantoms were configured in three ways: in the clinical concentration of the contrast agents that were administered to the patients, and those concentrations halved and doubled, respectively.
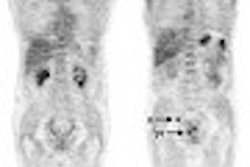
The authors found that that maximum error caused by CT contrast agent inducing an elevated FDG uptake in the PET image was 11.3%, with an average error margin of 4.4% to 2.8%. As for the phantom experiments, CT values that underwent the CT-to-PET transformation on the hybrid device produced elevated PET attenuation coefficients ranging from 2.5% to 26.2%. Overall, the study concluded that although oral CT contrast agents do cause SUV overestimation, these errors are not medically significant.
However, the group wrote that "it seems advisable to further develop the algorithms that transform CT values into PET attenuation coefficients. Improved methods must detect CT pixels representing oral contrast agents in a segmentation process and assign an adequate PET attenuation coefficient."
By Kate Madden YeeAuntMinnie.com contributing writer
June 20, 2003
Related Reading
Combidex aids in early lymph node metastasis detection, June 19, 2003
PET protocols from head to toe, May 5, 2003
German radiologists assess performance of PET-CT, March 10, 2003
In-line PET-CT system improves cancer diagnosis, March 10, 2002
Copyright © 2003 AuntMinnie.com