Wednesday, November 30 | 12:15 p.m.-12:45 p.m. | W5A-STCE-2 | Learning Center Theater
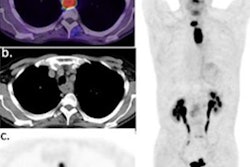
Nomograms may help guide the selection of the most suitable prostate cancer patients for F-18 DCFPyL-PET/CT (Pylarify) imaging, according to research presented in this session.Researchers at the U.S. National Institutes of Health gathered data on 199 patients with biochemically recurrent prostate cancer (median prostate-specific antigen [PSA] level of 2.0 ± 5.85 ng/mL) who underwent F-18 DCFPyL-PET/CT after either radical prostatectomy or radiation therapy. Scan positivity and disease location were correlated with variables including age, Gleason score, International Society of Urological Pathology (ISUP) grade group, primary therapy (radical prostatectomy vs. radiation therapy), positivity margin (for patients treated with radical prostatectomy), PSA doubling time (PSAdt), initial T-stage (< 3a or ≥ 3a), initial N stage, PSA at the time of the scan, and time from biochemical recurrence to scan.
A full-cohort multivariate regression analysis revealed that age, PSAdt, T-stage, and PSA are predictors for scan positivity and presence of extra-pelvic disease, with areas under the curve (AUCs) of 82% and 81%, according to the researchers. In the radical prostatectomy cohort, analysis revealed that original Gleason score, PSAdt, PSA, and months from biochemical recurrence to scan were predictors for scan positivity and presence of extrapelvic disease, with areas under the curve (AUC) of 0.84 and 0.80, respectively. In the radiation therapy cohort, the analysis revealed that PSAdt and PSA were predictors of extra-pelvic disease, with an AUC of 0.85.
"Nomograms to predict [F-18] DCFPyL-PET/CT scan positivity may reduce unnecessary medical and resource expenses for patients with high probability of a negative result," the group noted.