WASHINGTON - Israeli researchers yesterday gave SNM attendees a look at their research with an investigational SPECT/CT system that uses 64-slice CT integrated with a dedicated cardiac gamma camera. While they gave the system points for patient convenience, it's still unclear whether such a unit has a role in a clinical environment.
Hybrid imaging using integrated PET/CT systems has made dedicated PET cameras largely obsolete, but SPECT/CT is still developing its niche as clinicians investigate the best clinical applications for its mix of functional and anatomical information. A number of vendors currently offer SPECT/CT units in four-, six-, and now even 16-slice configurations, but no vendor has developed a commercial model matching the 64-slice units now available for PET/CT.
That's not to say no one is interested in 64-slice SPECT/CT. A fused SPECT/CT image produced by researchers from University Hospital Zurich in Switzerland was named Image of the Year at the 2006 SNM show. But that image was created by software that fused studies collected at different times on different scanners, rather than one session on a single dedicated SPECT/CT unit.
Researchers at Rambam Medical Center in Haifa began working with such a system in October 2006. The prototype unit pairs a 64-slice CT system (LightSpeed VCT, GE Healthcare, Chalfont St. Giles, U.K.) with a dedicated dual-head cardiac gamma camera (Ventri, GE). The imaging components share a common table and are aligned to enable sequential acquisition of registered data.
 |
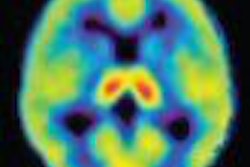
| Fusion myocardial perfusion/CTA image acquired with integrated SPECT/64-slice CT scanner. Image courtesy of Dr. Ora Israel, Rambam Medical Center. |
The study focused on myocardial perfusion, with the CT component providing anatomical information about coronary stenosis, localization, and severity, while SPECT provided detail on stenosis severity, according to Dr. Rachel Bar-Shalom, who presented the study at the SNM show.
Over a four-month period, the group studied 58 patients, of whom 25 were men and 33 were women, with a mean age of 57. All patients underwent the following imaging protocol:
- Single-day rest/stress SPECT myocardial perfusion with technetium sestamibi
- Low-dose CT for attenuation correction
- Exercise or pharmacological stress test
- Gated stress myocardial perfusion SPECT
- Low-dose CT for attenuation correction
- CT for calcium score and coronary CT angiography (CTA)
After a few patients were excluded for high or unstable heart rates, the group was left with 55 patients, in whom 215 coronary segments were evaluated, Bar-Shalom said. In the population, 83% of coronary segments in 56% of patients showed normal perfusion and coronary anatomy, Bar-Shalom said. Abnormal results were found in 13 segments in eight patients.
SPECT was negative for ischemia in 12 patients with 18 coronary segments that appeared narrow on the CTA study, while the CTA study was negative for significant coronary stenosis in four patients who had five ischemic segments.
Overall, the SPECT/CT data was of clinical value in 44% of patients, with hybrid SPECT/CT results used to guide further cardiac catheterization in eight patients who had both abnormal SPECT and CTA. Discordant SPECT/CT results, with either component negative, excluded the need for further procedures in 16 patients, Bar-Shalom said.
"Initial clinical data indicates that single-session SPECT/64-slice CT coronary angiography is a technically feasible, noninvasive modality for the concurrent assessment of the presence and significance of coronary artery disease," Bar-Shalom said.
In the question-and-answer portion of the talk, panel moderator Dr. Marcelo Di Carli of Brigham and Women's Hospital in Boston asked about the radiation dose delivered to patients in the study, which included two attenuation correction scans, a calcium score, and a CT angiogram, in addition to the SPECT -- especially an issue considering that over 50% of the patients in the study were normal.
Patients received doses ranging from 20-30 mSv, Bar-Shalom said, adding that the imaging protocols used were for research purposes, and that the researchers were using the results to debate which patient groups are most suited to receiving both studies.
An attendee in the audience suggested that one possibility would be to move the SPECT myocardial perfusion exam further up in the diagnostic workup, so that a CTA study would be conducted only if the SPECT were abnormal.
Another issue is whether SPECT/CT can be used to redirect patients from invasive coronary angiography -- typically the holy grail of cardiac imaging modalities. Di Carli said that this might not be the right question to ask, given that most patients with ischemia receive medical therapy rather than an intervention.
"The question is, can the CT information derive important prognostic data that will allow us to treat patients differently?" Di Carli said. "Can we refine our risk assessments that are based on perfusion by defining the burden of disease based on either the calcium score or the CT angiogram? Those studies will probably prove a better point for hybrid imaging than purely basing (its use) on who needs to go to cath."
The Rambam researchers plan to study the applicability of integrated SPECT/CT in patient groups with different risk factors in order to be more specific in terms of the patient populations that are scanned. The group also hopes to determine whether a combined SPECT/CT machine is truly needed in the clinical environment, or whether SPECT and CTA images can be collected on separate machines and fused later via software.
While the integrated unit is much more convenient for patients, "we aren't sure there is a need for a combined machine," Bar-Shalom said.
By Brian Casey
AuntMinnie.com staff writer
June 6, 2007
Related Reading
Study correlates CTA to angiography, myocardial perfusion SPECT, May 25, 2007
Instrumentation, attenuation correction steer nuclear cardiology's future, October 23, 2006
Cardiac SPECT/CT fusion captures SNM's Image of the Year, June 6, 2006
SPECT/CT implementation: More than plug and play, June 7, 2006
Copyright © 2007 AuntMinnie.com