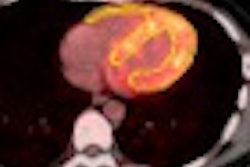
Hybrid PET/CT angiography (CTA) offers a full cardiac assessment in a single exam, compensating for each modality's weaknesses in heart imaging, according to results presented on Friday at the Society of Cardiovascular Computed Tomography (SCCT) meeting in Denver.
The hybrid acquisition can not only determine whether a coronary artery stenosis is anatomically significant, but also whether the blockage is flow-limiting and whether revascularization will be successful -- possibly avoiding invasive catheter-based angiography, researchers said.
"Our hypothesis was that we could noninvasively differentiate between ischemic and nonischemic cardiomyopathy without taking patients to the cath lab," said Dr. Nathan Dittoe, a cardiology fellow at Kettering Medical Center in Ohio, in an interview with AuntMinnie.com.
The retrospective study looked at 124 patients who were scanned using a hybrid PET/CT scanner (Gemini GXL, Philips Healthcare) equipped with 64-detector-row CT. The patient cohort (mean age, 59.5 ± 11.7 years; 60% male) presented with a variety of symptoms, but typically chest pain.
There were also a few healthy volunteers, making the cohort perhaps a little healthier than the general heart scanning population, Dittoe said. Mean body mass index (BMI) was 28.8, 20% of the patients were diabetic, 52% had hypertension, 32.5% were smokers, and 50.4% had dislipidemia. As for heart disease, 1.6% had congestive failures, and 13.8% had known coronary heart disease.
The total-body effective dose from CTA was 8.56 ± 4.9 mSv; with the addition of the nuclear medicine scan, this rose to approximately 14 mSv. The total time for the hybrid study was a little more than 30 minutes per patient.
All patients underwent an initial calcium scan, followed by rest and stress rubidium PET scans, followed by coronary CT angiography.
"We use a low-dose CT scan to line up the PET images so we're looking at the right field, so that when we send them through the PET scanner, we have an idea of where to put the windows," Dittoe said.
The investigators focused on patients with low ejection fraction (≤ 45%) as measured by the CT angiography portion of the test, but "we were hoping to find more patients with low ejection fraction than we did," he said.
The results showed that 50% of the cohort had both normal PET and CTA results, 10.5% had normal CTA but abnormal PET, 25% had abnormal CTA but normal PET, and 14.5% had both abnormal CTA and PET. Two patients had global hypokinesis.
Nine patients had low ejection fraction, and three (33%) of the nine had no stenosis or mild stenosis less than 40% in any vessel, constituting mild coronary artery disease. Following the group's hypothesis, a diagnosis of dilated cardiomyopathy was expected.
The CTA portion of the scan revealed that six (67%) of the nine patients with low ejection fraction had severe stenosis (≥ 70%) in at least one vessel. This group was examined with an eye toward potential ischemic cardiomyopathy.
Of these six, four had ischemia at PET and one showed scarring. "If you see scar on PET, you know revascularization will be unsuccessful because you can't revascularize dead tissue," Dittoe said.
The final patient of the six flagged by CT had severe three-vessel disease that was not identified by PET.
This last patient was a good example of why both modalities are needed for cardiac assessment: because the two modalities "compensate for each other's weaknesses," he said.
PET might be the stronger modality in patients with severe calcifications due to blooming artifacts at CT. However, PET will occasionally miss a patient with multivessel disease and so-called balanced ischemia, in which the patient has decreased perfusion to all areas of the heart, because PET is better at detecting the perfusion differences at single-vessel disease compared to the patient with global hypoperfusion.
The complementary nature of the modalities "saves you from having to make other decisions and send the patient for more invasive modalities," according to Dittoe.
"Hybrid PET/CT is feasible and rapid, we can do it in about 30 to 45 minutes without a whole lot of radiation exposure, and each modality is complementary to each other," as PET can help with perfusion and CT provides anatomic information, he said.
"We think that PET/CT can be used to determine the etiology of a patient's cardiomyopathy," Dittoe added. "So if a patient comes in with a low ejection fraction and a weak heart, we could send them for PET/CTA as their initial test of choice without the need for further exams, while determining if revascularization is helpful."
As opposed to simply doing a coronary CTA, the combined test might be indicated for a patient presenting with a weak heart or heart failure and no known coronary artery disease.
"We get more than diagnostic information, we get treatment planning out of this," he said.