
Like a golf ball perched on a tee, the glenohumeral joint in the shoulder is in a precarious position: Although it is amazingly agile, it's also unstable, rendering it prone to injury, impairment, and pain. By combining MR with a clinical exam, radiologists and orthopedists can take a look at the anatomy as well as the function of an abnormal shoulder joint.
Similar to the way functional MR has changed neuroimaging protocols, dynamic, real-time MR offers a wider spectrum of information about shoulder joint health, said Dr. Christopher Beaulieu in a presentation June 19 at "MR Advances in Musculoskeletal Imaging and Radiology," a conference hosted by Stanford University Medical Center. Beaulieu is an assistant professor of radiology at Stanford.
"If you think about joints, the function is to move us around. The glenohumeral joint has the widest range of motion of any joint in the body. Its stability is capsule- and ligament-based. We have a very oversized humeral head sitting on a glenoid. Disability and instability are common problems. By superimposing on the exquisite anatomic knowledge (obtained with MRI), we can start to look at function, and functional impairment, on a dynamic level." Beaulieu said.
At Stanford, an imaging technique has been developed that measures glenohumeral motion patterns as well as active joint motion. In a vertically open MR system (Signa SP, GE Medical Systems, Waukesha, WI), the patient sits perpendicular to the magnet bore. Images with a slice thickness of 7 mm are obtained with a fast gradient-recalled echo (GRE) sequence.
A specialized system, called MR Tracking, allows for active scan-plane registration. A miniature radiofrequency coil surrounds a sample of gadolinium solution. By adjusting the location of the coil on the patient, the scan location is modified.
"When you have a subject in the magnet, you apply the tracker coil in the area of interest on the shoulder," Beaulieu explained. "When he goes through and abducts his shoulder, we can follow the joint through a range of motion and, more or less, actively track the scan plane."
In one clinical example, Beaulieu described the imaging results for a 26-year-old female patient with chronic pain and instability in her shoulder.
"When she would abduct her arm at about 90 degrees, there was a very dramatic clunking sensation," he explained. "What she and her orthopedic surgeon assumed was that she would be in position as she abducted her shoulder and then it would inferiorly sublux. In fact, the MR showed the opposite was true. Early in abduction, the humeral head was subluxed superiorly to come in contact with the acromion."
Another option with this technique is to combine imaging with the clinical exam. While the patient is inside the magnet, the examiner applies force to the humeral head while scanning takes place.
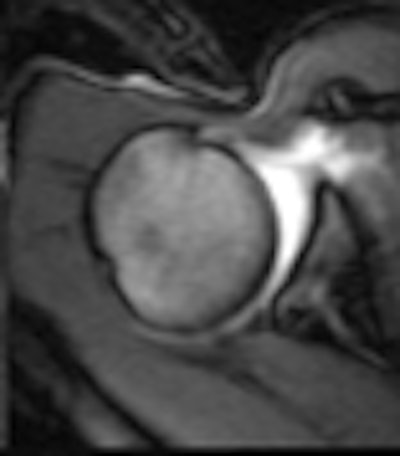
The photo above from Stanford depicts MR images during a stress test of an asymptomatic shoulder as the humeral head is moved from the center of the glenoid to a posterior position and back when force is applied.
"There's no radiation exposure to the patient or the examiner," Beaulieu said. "For the first time, perhaps, we can really connect the anatomic imaging with the physical examination, which can show us the pattern of instability."
Still, there are some disadvantages to dynamic shoulder MR. The specialized equipment is expensive, and the exam is time-intensive, particularly if it requires the orthopedic surgeon to be on-hand. But open scanners are becoming more common, and the Stanford group is striving for greater efficiency, Beaulieu said.
"Imaging plays a key role because clinical diagnosis is difficult even for advanced orthopedic surgeons. A physical exam may not give all the information that is needed. Static MRI and MR arthography don't always give the answers as to what's causing a patient's problems," he added. "This is information that can affect the surgical therapy that these patients undergo."
By Shalmali Pal
AuntMinnie.com staff writer
June 28, 2000
Let AuntMinnie.com know what you think about this story.
Copyright © 2000 AuntMinnie.com

















