Clinical diagnoses of acute musculoskeletal injuries aren’t always difficult to figure out, but pinpointing the degree and extent of injury can determine whether a patient will be out of commission for a few days or several weeks. By using MR to image osseous overuse and myotendinous injuries, radiologists can make that judgment call, according to two presentations at the recent "MR Advances in Musculoskeletal Imaging" conference hosted by Stanford University of Stanford, CA.
Dr. Christopher Beaulieu, an assistant professor of radiology at the university, discussed his department’s use of MR to diagnose osseous overuse injuries, which can theoretically be divided into two categories. Fatigue fractures generally occur when normal bone responds to supernormal forces over time, as in professional long-distance athletes who may run as much as 70 miles a week. Insufficiency fractures come about when abnormal bone that has been weakened by age or disease is subjected to relatively normal physiologic forces.
"In reality, there is a blurring between these two categories," Beaulieu said at the June meeting in San Francisco. "On the one hand, you have older individuals who are becoming more active. On the other hand, you have younger individuals who should have normal bone, but may have other risk factors." The "weekend warrior" athlete or patients with nutritional issues would be examples of the latter, he added.
"In either case, the build up of abnormal fluid is the key, and MR is particularly adept at spotting edema, which can be found in the periosteal region or the endosteal region of the bone, or in the cancellus bone marrow," he said.
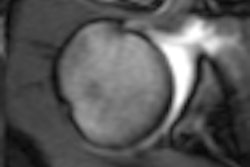
For sensitivity to marrow or periosteal edema, Beaulieu recommended fat-suppressed T2-weighted imaging in addition to T1-weighted images. The scanner should be capable of either homogeneous chemical fat suppression or short T1 inversion-recovery imaging (STIR), he wrote in the conference syllabus. If fat suppression is inhomogeneous, fast-STIR echo can be used on a 1.5-tesla scanner. Beaulieu said he preferred chemical saturation or water-selective excitation to inversion recovery because of the higher signal-to-noise ratio and superior image quality. The image above illustrates a typical stress fracture of the sacrum.
"When you are looking for fractures, what you want to look for are those linearities that are within the center of the marrow edema. The geographic edema, if we only saw that, we would call it a stress reaction. But once we saw a low signal line, we would upgrade and call it a stress fracture," he said. "Why is that important? It turns out that along the spectrum from a stress reaction to a stress fracture, the recovery time [becomes] much higher. If you identify [the degree of stress] early on, you can help stage these injuries."
In a second presentation, Dr. William Palmer from Massachusetts General Hospital in Boston talked about imaging and myotendinous (MT) injuries, or the "MRI of pains and strains," he said. Palmer is the chief of bone and joint radiology at the hospital.
"Whether you fall into the category of a competitive athlete or a ‘weekend warrior,’ nearly everyone has had some sort of muscular tendon injury, he said. Most people experience late muscle soreness, which arrives a day or two after strenuous activity. Acute myotendinous strain is the "immediate onset of pain and discomfort during exercise."
The two goals of the myotendinous imaging protocol are to identify, localize, and characterize abnormalities in the myotendinous unit, as well as distinguish injury from inflammatory disorders or neoplasms.
In Palmer’s estimation, both long- and short-axis imaging should be performed. In the coronal or sagittal plane, T1-weighted and STIR sequences show the extent and length of lesions. STIR images also optimize contrast resolution and help detect subtle lesions. The field-of-view should be large enough to include the tendons of either origin or insertion in affected muscle groups.
"The major point I want to make is that within the myotendinous unit, the MT junction represents the weak link, and the location where sprain injuries classically occur," Palmer said.
In the axial plane, proton density and T2-weighted sequences should be obtained using a smaller field-of-view.
"On T1-weighted images, the surrounding proximal tendon is a region of high signal that’s mildly heterogeneous. On T1-weighted images, there are relatively few things that can be high signal. Fat is one and hemorrhage is another," Palmer said.
Immediately following the least severe strain, MR scans will show interstitial edema and hemorrhage that is centered on the MT junction and then spreads into the surrounding muscle. In second-degree strains, a partial tear of the MT fibers occurs and MR findings include hematoma in the MT junction, interstitial edema, and hemorrhage.
As with osseous overuse injuries, chronic disorders of the MT unit develop over time and include tenosynovitis, tendinopathy, and rupture, Palmer said. When doing MR scans on these patients, clinicians should watch out for lesions that contain fat, such as hemangioma, which look similar to hematoma and may masquerade as an acute injury.
MRI of osseous overuse and MT unit problems does have certain diagnostic pitfalls. Myositis ossificans can simulate an inflammatory mass and lead to unnecessary needle biopsy or surgical resection. Beaulieu pointed out that such lesions as transient osteoporosis and osteomyelitis can look identical to stress injuries.
By Shalmali Pal
AuntMinnie.com staff writer
July 28, 2000
Let AuntMinnie.com know what you think about this story.
Copyright © 2000 AuntMinnie.com