Researchers have combined MR imaging with blood-pressure monitoring for a noninvasive assessment of aortic pressure-area curves -- an approach that may distinguish those patients with Marfan syndrome who will benefit from beta-blocking agents.
Beta blockers can reduce the rate of premature aortic dilatation and dissection in patients with Marfan syndrome, a congenital disorder that can lead to a fatal rupture of the aorta. However, some patients experience no benefit from beta-blocking drugs, and may even be harmed by them.
In a new study, Dutch researchers hypothesized that differences in aortic pressure-area curves may explain the heterogeneous response to beta blockers. The study, led by cardiologist Dr. Barbara Mulder of the Academic Medical Centre in Amsterdam, is published in the latest issue of Heart (March 2004, Vol. 90:3, pp. 314-318).
The study also allowed the researchers to use their novel noninvasive approach to measuring pressure-area curves. Other approaches involve intravascular measurements or transesophageal echocardiography with aortic-pressure measurement or brachial pressure measured by a sphygmomanometer.
The researchers looked specifically for a transition in the pressure-area curves from a linear to an exponential course -- marking a move from aortic elasticity to stiffness.
"This transition point is a denominator of aortic elastic behavior in the normal blood pressure range, and is of additional importance in relation to the forces the aorta can withstand before rupturing," the authors wrote.
 |
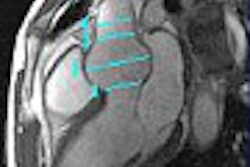
MR image of aortic site at which the pressure-area curve was constructed. The arterial-pressure waveform is usually almost identical to the aortic-area waveforms. The area waveforms assessed by MRI were then matched in time with the reconstructed aortic-pressure waveform. Image and caption courtesy of Dr. Barbara Mulder.
A total of 42 subjects -- 32 with Marfan syndrome and 10 controls -- were examined using a Siemens Magnetom Vision 1.5-tesla scanner (Siemens Medical Systems, Erlangen, Germany), followed by arterial blood recording using a Finometer finger monitor (Finapres Medical Systems, Arnhem, the Netherlands).
The entire aorta was imaged in the transverse and oblique sagittal planes using a standard spin-echo pulse sequence. A high-resolution gradient-echo pulse sequence with a velocity-encoding gradient was then applied perpendicular to the aorta, the authors reported, resulting in multiphase image pairs of modulus- and velocity-encoded images with a temporal resolution of 24 ms through the cardiac cycle, and spatial resolution of approximately 1 pixel/mm.
Reconstructed aortic blood pressure and area waveforms were assessed at the descending thoracic aorta at the level of the pulmonary bifurcation, the authors wrote, allowing for the inclusion of Marfan patients with aortic root replacements in the study.
"Aortic blood pressures can only be recorded invasively, and reconstruction techniques are helpful tools to estimate more central pressures from noninvasive recordings," the authors wrote. "As it is not yet possible to use the Finometer front end in the MRI scanner, pressure recording was done immediately after imaging."
No transition point was seen in the pressure-area curves for any of the control subjects and for most of the Marfan patients, regardless of their beta-blocker status.
"However, in six of the 32 patients with the Marfan syndrome (19%), a transition point in the pressure-area curve was demonstrated," the authors noted. "In these patients the transition point was shifted to much lower pressures, which could indicate more pronounced degeneration of the medial layer of the aortic wall than in patients without a transition point."
"This suggests that the presence of a transition point in the pressure-area curve could play a role in the heterogeneous response to beta-blocker treatment in relation to the elastic properties and dilatation rate," the researchers added. Others have reported that in some patients with moderate-to-severe dilatation of the aortic root, aortic properties worsened during beta-blocker treatment.
Because Marfan patients regularly undergo MRI for monitoring aortic dimensions, the authors noted, their measurement approach isn’t stressful to patients and likely wouldn’t affect their blood pressure.
"Adaptation of the Finometer device to ensure reliable function in the strong magnetic field of the magnetic resonance scanner -- combined with new developments in
MRI as ‘real time,’ or techniques with a smaller temporal resolution -- will further improve the noninvasive assessment of pressure-area curves in the near future," they concluded.
By Tracie L. ThompsonAuntMinnie.com staff writer
March 2, 2004
Related Reading
Myocardial ischemia, viability made apparent with MR, February 6, 2004
ISET talks offer innovative ways to survey aortic aneurysm repair, January 30, 2004
Doppler measurements of hemodynamic factors aid in trauma case management, October 16, 2003
Ultrasound test could help prevent sudden death in athletes, June 19, 2000
Copyright © 2004 AuntMinnie.com