Radiation risks have taken the sheen off CT for whole-body screening. But MRI, with no major health concerns, may yet succeed, researchers from Germany report. Their findings show that multiorgan MRI screening exams are technically feasible.
The study from the University Hospital Essen in Germany is among the first to implement and evaluate a comprehensive MRI-based screening exam. The researchers found that the exam detected signs of atherosclerotic disease in 21% and peripheral vascular disease in 12% of the study population, which consisted of 298 asymptomatic patients (American Journal of Roentgenology, February 2005, Vol. 184:2, pp. 598-611).
Twelve colon polyps, nine pulmonary lesions, two cerebral infarctions, and one myocardial infarction were also discovered, apart from findings in nontargeted organs. There was one false-positive case and one minor allergic reaction.
The study authors, however, do not recommend full-body MRI screening outside a research setting. "Our recommendation is not to advertise this to the population, but to first undertake long-term studies to see if the benefits outweigh the potential risks," said lead author Dr. Susanne C. Goehde.
The potential risks relate to the usefulness of screening and the debate about its benefits. "The scanning gives a dramatic bundle of information. Although one might think that this increases health in the future, there is controversy," Goehde said.
Multiorgan screening
The brain, arterial system, heart, and colon were the target organs included in the screening study. Imaging was performed on a 1.5-tesla Magnetom Sonata system (Siemens Medical Solutions, Erlangen, Germany), with a rolling table platform (AngioSURF, MR-Innovation, Essen, Germany) for whole-body coverage.
The whole exam can be completed in a little over an hour, with time savings facilitated by the sliding-table concept and the use of high-performance gradients, the authors reported. The exam consisted of cerebral MRI, MR angiography (MRA), pulmonary MRI, cardiac MRI, and MR colonography (MRC).
Clinical examination, therapy, or further diagnostic workup confirmed most (75%) of the relevant findings.
Cerebral MRI
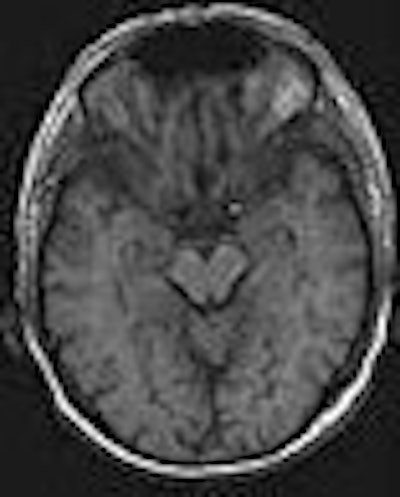
The cerebrum was assessed by T1- and T2-weighted fast spin-echo, FLAIR, and diffusion-weighted imaging. The intracerebral arterial system was directly visualized by axial 3D time-of-flight MR angiography.
The authors reported high accuracy for screening for myocardial infarcts. "On the basis of delayed enhancement, infarcted myocardium is detected on T1-weighted images with high sensitivity and specificity, allowing early secondary prevention strategies that have been shown to alter outcomes in high-risk, not-yet-symptomatic patients," they wrote.
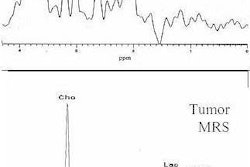
Screening for cerebral tumours was done using a contrast-enhanced cerebral sequence. Repeat administration of contrast was avoided by performing the scan after the cardiac exam, so the contrast administered for MR angiography was also used for the cerebral sequence.
 |
| Fifty-one-year-old male smoker with hyperlipidemia. T1-weighted FLASH image of brain parenchyma shows normal findings (AJR 2005; 184:598-611). |
MR angiography
MR angiography was based on five slightly overlapping 3D coronal datasets (64 sections each) acquired in immediate succession using a 3D FLASH sequence. Each dataset was collected over 12 seconds, with the first three using the breath-hold technique.

After conventional test bolus timing with 1 mL at 1.2 mL/sec for individual assessment of circulation time, a 1-molar gadolinium-based contrast agent (gadobutrol, Gadovist 1.0, Schering, Berlin) was administered at a dose of 0.2 mmol/kg of body weight for arterial enhancement. The contrast material was diluted with saline solution to a total amount of 60 mL. Then, a biphasic contrast injection protocol was used: a first flush of 30 mL at 1.2 mL/sec and a second flush at 0.7 mL/sec, followed by a saline flush of 20 mL at 0.7 mL/sec. No venous compression was used, the authors wrote.
Whole-body MR allows rapid evaluation of the lower peripheral arterial system (AJR, June 2004, Vol. 182:6, pp. 1427-1434). However, one of the drawbacks of MRA is that lumen of the coronary arteries is not assessed. "Even though several techniques have been proposed, none has gained clinical relevance," the authors stated.
Pulmonary and cardiac MRI
To depict pulmonary parenchyma and the cardiac morphology, axial HASTE imaging (slice thickness of 8 mm) of the thorax was performed. Two blocks of slices were acquired using the breath-hold technique. Functional assessment of the heart was also done at a later stage.
To overcome artifacts while depicting the lungs, ultrashort TEs were used. However, small calcified nodules and lesions less than 3 mm in diameter were missed because of lack of signal-providing protons.
The authors recommended that screening for pulmonary nodules should be also included in the exam, given that lung cancer is a leading cause of cancer death, and that early detection can lead to better outcome.
MR colonography
Bowel cleansing was done for MR colonography, and 40 mg of scopolamine was administered intravenously to minimize bowel motion. Glaucoma required the alternative use of glucagon in three subjects (dosage 100 mg = 1 IU). Imaging was done in the prone position, the authors wrote.
The colon was filled with 1,500-2,500 mL of warm tap water via rectal enema. No fluoroscopic imaging was performed. T1-weighted 3D gradient-echo images (96 sections) of the colon were collected during breath-holding over 23 seconds before and 60 and 90 seconds after a second intravenous administration of gadobutrol at a dose of 0.1 mmol/kg of body weight.
"MR colonography overcomes many of the shortcomings limiting the clinical impact of existing screening techniques, including the gold standard conventional colonoscopy," the authors wrote. For MRC, the technique used was the setting of a dark, water-filled colonic lumen with lesion detection based on enhancement of the colonic wall and of colorectal masses.
 |
| Seventy-three-year-old man with history of polypectomy. Coronal source image of 3D gradient-echo dataset shows small polyp in ascending colon (arrow) (AJR 2005; 184:598-611). |
Findings in nontargeted organs
The research group also detected relevant findings outside the target organs, mostly in the abdomen. The findings included a case of renal cell carcinoma.
"Analysis of the parenchymal organs in the abdomen can be based on 3D gradient-echo datasets collected in the arterial, portal venous, and hepatic venous phases. The first dataset is provided as part of the whole-body MR angiography examination, and the subsequent datasets are collected for MR colonography," the authors wrote.
The future of MRI screening
"The incidence of relevant findings in an asymptomatic population identified in both targeted and nontargeted organs was high, and underscores the potential impact of an MRI-based screening strategy," the authors concluded.
Cost-benefit concerns and potential harm from treating false-positive cases were outside the scope of the study. What the study does offer, however, is a design for potential large-scale MRI-based screening exams in the future.
By N. Shivapriya
AuntMinnie.com contributing writer
February 10, 2005
Related Reading
Whole-body MR may be feasible for tumor staging, August 28, 2002
Multiorgan MRI/MRA screening finds unsuspected pathology, April 18, 2002
MRA gauges spiral blood flow as predictor of renal deterioration, March 2, 2002
AngioSURF rides new wave in MR angiography, April 11, 2001
Copyright © 2005 AuntMinnie.com