In a new study by researchers from the U.K., 1.5- and 3.0-tesla MRI showed strong agreement in both mass and transmural extent of myocardial hyperenhancement (HE) when using the same segmented inversion-recovery turboFLASH pulse imaging sequence for patients with previous myocardial infarction (MI).
The study, although limited to 16 patients (all men, mean age 66 ± years), showed that delayed-enhancement (DE) MR imaging at 3 tesla is a reproducible technique for differentiating irreversible injury from viable myocardium.
"Results of studies have demonstrated the effectiveness of a segmented inversion-recovery fast gradient-echo ... MRI sequence to help differentiate irreversibly injured myocardium from normal myocardium, with signal intensity (SI) differences of nearly 500% obtained with 1.5-tesla systems," wrote principal investigator Dr. Adrian Cheng from the University of Oxford and John Radcliffe Hospital in Oxford, U.K. "This technique of delayed-enhancement MR imaging has been shown in animal and human studies to depict the presence, location, and extent of acute and chronic irreversible myocardial injury in those with coronary disease" (Radiology, January 5, 2007).
MR is not only superior to SPECT for identifying the transmural extent of irreversible injury, it enables identification of even the smallest areas of myocardial necrosis, they added.
Now that 3-tesla MRI systems are available, with their superior signal-to-noise ratio and potential to improve applications that have been hampered by low spatial and temporal resolution, the question arises as to whether the results for these applications will correspond to 1.5-tesla MRI studies using the same application.
Cheng and his colleagues Matthew Robson, Ph.D.; Dr. Stefan Neubauer; and Joseph Selvanayagam, Ph.D., aimed to prospectively compare visualization and quantification of irreversible myocardial injury at both 1.5- and 3.0-tesla systems in patients with chronic MI. Infarction was confirmed with elevated troponin levels combined with clinical history and/or previous imaging results. Only patients with standard contraindications to MR imaging were excluded.
All patients were imaged twice in random order and by the same operator using the same imaging sequence at 1.5- and 3-tesla (Sonata and Trio, respectively, Siemens Medical Solutions, Malvern, PA).
Short-axis cine images covering the left ventricle (LV) were acquired using a retrospectively electrocardiographically gated steady-state free precession frequency pilot "to aid delineation of the subendocardial border" when matched with contrast-enhanced images. Gadolinium-based contrast (0.1 mmol/kg of body weight) was administered intravenously, followed by a saline flush.
Short-axis images of the left ventricle were acquired with a breath-hold T1-weighted segmented inversion-recovery turboFAST low-angle shot (FLASH) sequence (flip angle 50°, repetition time 25.6 msec at 1.5 tesla and 26.7 msec at 3.0 tesla). Two experienced readers working in consensus determined the T1 that best nulled the signal of the normal myocardium.
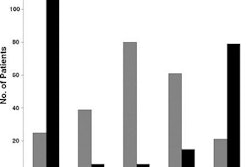
A Bland-Altman analysis showed no systematic bias in HE mass (mean difference, 0.2 g; 95% CI: -0.7 g, 1.2 g) and acceptable limits of agreement (-3.3 to 3.8 g) between the two field strengths. The HE mass measurements were also strongly correlated (R² = 0.99). No significant difference was seen in measurements at 1.5 and 3.0 tesla (28.1 g ± 15.7 [22.6% ± 10.9 of LV mass] versus 27.8 g ± 15.7 [22.3% ± 10.7 of LV mass], respectively (p= 0.5999).
And there was high agreement in all field strengths for HE detection (k = 0.90) and transmural grade (k = 0.79), and intra- and interobserver variability was low for both scanners. The initial inversion time chosen to null the signal of the normal myocardium was 57 msec ± 20 longer at 3.0 tesla compared with 1.5 tesla.
The same turboFLASH MR pulse sequence yielded a strong agreement in both mass and transmural extent of myocardial hyperenhancement between the two field strengths, Cheng et al wrote.
Two elements are critical in the clinical performance of the delayed-enhancement MR at 1.5 tesla, the authors noted. "First, its ability to quantify small areas of myocardial necrosis (with resolution almost 30-fold greater than that at SPECT) allows visualization of microinfarcts that cannot be depicted with other imaging techniques," they wrote. Second, the technique provides information about the transmural extent of irreversible injury, "which makes it a powerful tool for the prediction of myocardial viability."
These two measures were virtually identical between the two field strengths "despite sternal wires and coronary stents in a substantial proportion of patients, and despite theoretic concerns of reliable R-wave triggering ... at 3.0 tesla."
The low intra- and interobserver variability shows that the technique is reproducible at both field strengths as well, they added.
There was less agreement for transmural grade of hyperenhancement than for detection of hyperenhancement, they noted, due to inherently greater variability in scoring transmural grade from 0 to 4 when compared with that of the binary decision as to whether hyperenhancement is present, as well as some variability in segment registration.
Injured myocardium shows greater shortening of T1 after contrast enhancement compared to normal myocardium, and at 3.0 tesla myocardial T1 is inherently longer than at 1.5 tesla. For this reason, "optimal T1 to null the signal of normal myocardium needs to be longer at 3.0 tesla" at the same time of contrast administration.
Limitations of the study include a small patient cohort and residual contrast remaining during the second imaging study in each patient, which may have affected T1 and/or mass of the hyperenhancement, the authors stated.
"We envisage that (delayed-enhancement) MR can be included as part of the comprehensive cardiac MR protocol at 3.0 tesla with applications such as myocardial perfusion and spectroscopy that are likely to be improved by the increased signal-to-noise ratio associated with the higher field strength," they wrote.
By Eric Barnes
AuntMinnie.com staff writer
March 15, 2007
Related Reading
Real-time 3DTTE comparable to MRI in LV evaluation, February 28, 2007
Bosentan improves myocardial function in systemic sclerosis patients, January 18, 2007
Drug-eluting stents reduce subsequent MI frequency and mortality, February 22, 2007
Drinking coffee seen not to increase the risk of myocardial infarction, February 14, 2007
Copyright © 2007 AuntMinnie.com