![]()
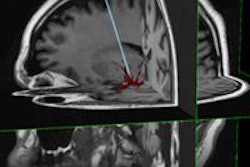
Image-guided radiotherapy (IGRT), and the evolution of the technique over the past 20 years, was the subject of a keynote presentation at the SPIE Medical Imaging conference held February 13-18 in San Diego. "We've seen a transition from a technique-based approach to employing 3D information in creating the intervention," explained David Jaffray, Ph.D., head of radiation physics at Princess Margaret Hospital in Toronto.
In the opening address of the meeting's "Physics of Medical Imaging" track, Jaffray described how the introduction of highly conformal radiotherapy modalities increased the need for precision targeting. Considering the fact that patients move and targets morph over the course of fractionated therapy, co-location of target and therapeutic dose distribution poses a significant technical challenge.
"It's not just a case of getting it right once, it must operate reliably over several weeks," he explained. "In-room image guidance is a necessary development in the push toward dose escalation and normal tissue avoidance in radiotherapy."
Quality control
Imaging provides accurate measurement of patient position within the treatment room and enables verification of patient setup against planned geometry. Highly integrated IGRT systems are available and in clinical use, with substantial deployment of volumetric IGRT seen over the past five years. At Princess Margaret Hospital, for example, online conebeam CT guidance is now used for around 70% of cases.
Jaffray discussed the close relationship between imaging and quality assurance, noting that the most impact could likely be upon lung cases treated with stereotactic body radiotherapy. Here, online image guidance with conebeam CT can almost completely eliminate target positioning errors.
As well as increasing the accuracy of patient setup and radiation delivery, Jaffray suggested that imaging information can be used to redesign the treatment plan, on the basis of therapy-induced changes, for example. He cited an example study comparing radiotherapy for head-and-neck cancer with and without adaptive treatment planning. Weekly adaptation delivered a better dose to the target, as well as enabling the use of tighter margins and, thus, substantially lowering the parotid dose.
"Adaptive replanning provides a huge opportunity to reduce the amount of normal tissue irradiated, while retaining minimum target dose," Jaffray noted.
MRI guidance
So what's next for IGRT? According to Jaffray, the future may lie in the integration of MR guidance. MRI provides excellent soft-tissue contrast without exposing the patient to ionizing radiation. It also offers physiological measurement capabilities. Potential drawbacks include the effect of the magnetic field on dose deposition, as well as system expense, Jaffray noted. "We've seen a great interest develop in the joining of MR systems and radiotherapy," he said.
Several MR-guided radiation treatment systems are currently under development. For example, a team headed by Gino Fallone, Ph.D., director of medical physics at the Cross Cancer Institute in Edmonton, Alberta, has designed an instrument in which a linac and a 0.2-tesla MRI magnet are mounted on a gantry that rotates around the patient. In this "rotating-biplanar" geometry, the beam and field are fixed with respect to each other. In March 2009, Fallone's team demonstrated the first MR imaging during photon irradiation.
An alternative design, and an approach being investigated by medical physicist Jan Lagendijk, Ph.D., and colleagues at the University Medical Center Utrecht in the Netherlands, is to fix the magnetic field with respect to the patient. The Utrecht system uses a higher field strength of 1.5 tesla. The researchers have already demonstrated that MR imaging with the radiation beam switched on does not degrade the performance of either the linac or the MR scanner.
Jaffray also mentioned the Renaissance system under development by Jim Dempsey at ViewRay (Oakwood Village, OH). This device combines MRI with gamma radiotherapy, using three Co-60 sources with multileaf collimators. Elsewhere, Dr. Tomas Kron, professor of radiotherapy at the Peter MacCallum Cancer Centre in Melbourne, Australia, is also working on a cobalt-based treatment system, integrating MRI guidance with helical tomotherapy delivery.
At the Princess Margaret Hospital, meanwhile, Jaffray and colleagues are employing active MRI guidance for radiotherapy using a Siemens 1.5-tesla MRI on rails. Here, the MRI system is moved into the radiotherapy treatment room, imaging is performed, and the MRI is then removed. "We can do this today," he pointed out.
Jaffray concluded that MRI-guided radiotherapy appears to be feasible, both from an engineering and a physics perspective. Ongoing challenges include establishing the predictability of dose delivered in a magnetic field, as well as logistical and safety issues. "I think we'll see MRI-guided radiation treatment systems on the market within a few years," he predicted.
By Tami Freeman
Medicalphysicsweb editor
May 20, 2010
Related Reading
IGRT boosts outcomes for obese prostate cancer patients, September 3, 2009
© IOP Publishing Limited. Republished with permission from medicalphysicsweb, a community Web site covering fundamental research and emerging technologies in medical imaging and radiation therapy.