
Sophisticated histogram-based measurements of diffusion on MRI scans can predict bladder tumor aggressiveness noninvasively, according to a new study in Abdominal Imaging. The results could potentially help clinicians tailor therapy to individual patients, and even help predict which patients' tumors will metastasize.
The study included patients with bladder cancer who had an MRI before undergoing radical cystectomy. Results showed that one of the measurements, mean apparent diffusion coefficient (ADC), was significantly lower in patients with advanced cancers (stage T3 and higher) than in those with lower-stage tumors.
In addition, measurements of kurtosis, another advanced metric based on ADC, were significantly lower in patients with nodal disease, and kurtosis also trended lower in the subset of patients who later developed metastases, the researchers from NYU Langone Medical Center reported (Abdom Imaging, August 13, 2014).
 Dr. Andrew Rosenkrantz from NYU Langone.
Dr. Andrew Rosenkrantz from NYU Langone."We found that the combination of metrics had strong potential for predicting the aggressiveness and behavior of bladder cancer," said lead author Dr. Andrew Rosenkrantz in an interview with AuntMinnie.com. "Mean ADC is a standard metric that's been the most widely used, but we found that by using this more sophisticated, more quantitative algorithm, we could improve on standard diffusion metrics to give a more complete and more accurate characterization of bladder cancer outcomes."
Substantial variability
Bladder cancer is a common disease, accounting for some 15,000 deaths per year in the U.S. But it is also heterogeneous, with substantial variability in disease extent, aggressiveness, and prognosis among patients. Five-year survival is 96% for tumors without muscle invasion, but the rate drops to 70% when invasion is present.
Treatment selection and disease stage and grade are critical determinants of outcome, but with current diagnostic methods, it's not always clear to clinicians what they're dealing with. MRI and biopsy generally reveal the extent of disease and point the way toward treatment, but these tools aren't perfect, said Rosenkrantz, who is an assistant professor of radiology.
"Sometimes patients haven't been biopsied yet, or the biopsy can be wrong," he said. One key question is whether the tumor is invading the muscle layer of the bladder wall, because these patients have worse outcomes, he said.
A number of published studies have used MRI to investigate this question; however, Rosenkrantz and colleagues also wanted to look at factors such as metastasis to lymph nodes and other organs, as they were looking at the behavior and prognosis of these tumors to find the most aggressive ones using more advanced or quantitative MRI measures.
The 23 bladder cancer patients in the study (21 men, 2 women; mean age, 70 ± 11 years) underwent MRI on a 1.5-tesla scanner (Magnetom Avanto, Sonata, or Symphony; Siemens Healthcare) or, in one case, on a 3-tesla machine (Magnetom Trio, Siemens) before cystectomy. The patients received standard T1- and T2-weighted imaging, along with axial diffusion weighted imaging (DWI) of the bladder using a single-shot fat-suppressed echo-planar imaging technique. Repetition time (TR)/echo time (TE) was 2,000-2,800/76-83 msec, field-of-view was 350-400 mm, and slice thicknesses was 6-8 mm.
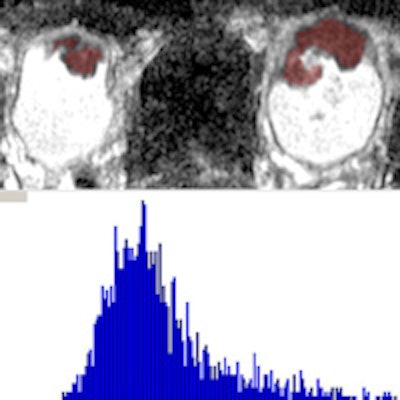
From these images, the researchers created ADC maps on a voxel-by-voxel basis for analysis using a standard monoexponential approach. They placed a volume of interest on all slices on the ADC map that encompassed each lesion, measuring whole-lesion mean ADC, kurtosis, and skewedness of ADC. They then compared this with T stage and pelvic nodal status at cystectomy, and later with subsequent metastasis in the 20 patients who presented for follow-up.
 Top of image shows consecutive slices from axial ADC map in patient with an anterior bladder tumor. Red overlay indicates portion of a whole-lesion volume of interest (VOI) encompassing the tumor. Bottom portion shows the histogram from this VOI, which was used to determine the mean, kurtosis, and skewedness of the whole-lesion ADC. Image courtesy of Dr. Andrew Rosenkrantz.
Top of image shows consecutive slices from axial ADC map in patient with an anterior bladder tumor. Red overlay indicates portion of a whole-lesion volume of interest (VOI) encompassing the tumor. Bottom portion shows the histogram from this VOI, which was used to determine the mean, kurtosis, and skewedness of the whole-lesion ADC. Image courtesy of Dr. Andrew Rosenkrantz.One limitation of ADC has been the method of evaluating it: Traditionally, a single region of interest is placed somewhere on the tumor in a single image slice, but this technique is prone to sampling error and incomplete evaluation, the study team wrote. The whole-lesion ADC histogram used for the current study requires placing a volume of interest that encompasses the tumor on every image slice on which it appears, providing a more sophisticated and comprehensive assessment, including metrics that examine lesion texture.
The group used in-house software called FireVoxel, which "was helpful for doing the whole-lesion evaluation, as well as for obtaining the histogram metrics," Rosenkrantz said. The software's capabilities for efficiently measuring the various parameters of a histogram aren't available on a standard PACS, but its functionality could generally be recreated by an experienced programmer, he noted.
Bladder cancer aggressiveness
Because whole-lesion ADC metrics have shown value in other pelvic malignancies, the group hypothesized that they could be used to measure bladder cancer aggressiveness. Rosenkrantz and colleagues therefore aimed to explore the associations between whole-lesion histogram diffusion metrics and pathologic findings and the development of metastases in bladder cancer patients.
At radical cystectomy, nine (39%) of the 23 patients were classified as stage T2 and 14 (61%) were stage T3 or greater; five (28%) patients exhibited nodal metastatic disease at cystectomy. Among the 20 patients with available postoperative imaging, seven (35%) developed metastatic disease. Histogram analysis revealed the following:
- Mean ADC was significantly lower in patients stage T3 and greater, compared with lower stages (p = 0.044), but it did not show an association with nodal or metastatic disease (p = 0.362-0.709).
- Kurtosis was significantly lower in tumors with nodal disease, versus those without (p = 0.037), and it showed a nonsignificant decrease in tumors with later metastases, compared with those without metastases (p = 0.088).
- Kurtosis was not associated with T stage (p = 0.811), and skewedness was not associated with any outcomes (p = 0.516-0.643).
"At ROC analysis, mean ADC achieved the highest area under the curve (AUC) for identification of stage ≥ T3," the authors wrote. "However, kurtosis achieved the highest AUC both for nodal disease ... and for later metastases."
Still, except for kurtosis' significantly higher AUC for the prediction of nodal disease versus skewedness, the differences in AUC between metrics weren't statistically significant, they cautioned.
The results showed that some of the limitations of standard ADC measurements used in past studies could be overcome with better measurement parameters.
"More complex ways of processing data gave us a more sophisticated measurement of kurtosis," Rosenkrantz said. "We took the standard acquisition, but we processed it with advanced software to obtain more comprehensive metrics, and those panned out as providing additional value."
Previous studies had not explored complex, whole-lesion analysis in bladder cancer, he said. Still, patient numbers were low, and the study was therefore underpowered to provide really reliable prognoses, especially for the prediction of future metastases, of which the current group had only seven.
But these shortcomings can be fixed with larger cohorts, he said. The plan is to perform a larger study that is also conducted at more than one center.
"We intend for our findings to ultimately be useful clinically for improving determination of patient prognosis and treatment selection in bladder cancer," the authors wrote.
"There is an increasing range of therapies being used for bladder cancer, treatment options are becoming more complex, and choosing among the various options can be difficult and complex," Rosenkrantz said. "If our metrics can be validated, it can help in making these decisions."

.fFmgij6Hin.png?auto=compress%2Cformat&fit=crop&h=100&q=70&w=100)



.fFmgij6Hin.png?auto=compress%2Cformat&fit=crop&h=167&q=70&w=250)










