Quantitative imaging biomarkers (QIBs) are a promising approach for evaluating normal biological or pathogenic processes, as well as response to treatment and intervention without the need for additional invasive procedures. Using QIBs in clinical and research domains may significantly improve diagnostic accuracy and patient outcomes, especially for complex and chronic diseases.
Nonalcoholic steatohepatitis (NASH) offers a great example of the application of quantitative imaging biomarkers for medical image analysis and overall clinical application. NASH can be called a "transition" disease, as it develops from nonalcoholic fatty liver disease (NAFLD) and can then progress to cirrhosis. Moreover, patients with early-stage nonalcoholic steatohepatitis have an 18% to 39% chance of developing more advanced stages of hepatic fibrosis within three to eight years, which significantly increases the condition's overall burden on the liver.
NASH diagnosis standard
Liver biopsy is a standard procedure for NASH diagnosis and staging. However, biopsy has a number of disadvantages, including the following:
- Sampling error
- Intra- and interrater variability
- Poor patient acceptance
- Potential complications (such as excessive bleeding and death)
Due to these disadvantages, liver biopsy is not considered optimal for screening, monitoring, and clinical decision-making for NASH patients. Therefore, there is a need to provide healthcare organizations with a noninvasive -- yet accurate -- alternative.
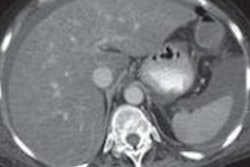
Quantitative imaging biomarkers are noninvasive and can reliably reflect fat content in liver parenchyma, allowing providers to detect, grade, and monitor NASH. To calculate and measure liver biomarkers, MR techniques such as MRI, MR spectroscopy (MRS), and MR elastography (MRE) are used. Ultrasound and CT are proposed by some researchers as well; however, these modalities have limited accuracy in accessing liver fat.
An additional advantage of MR techniques is that they can decompose liver signals into fat and water signal parts, which allows the assessment and quantification of liver fat more accurately than ultrasound or CT, with the higher chance of distinguishing inflammation and fibrosis from steatosis.
MRI-based QIBs
Magnetic resonance quantifies hepatic steatosis by measuring the proton density fat fraction (PDFF). PDFF is the fraction of MRI-visible protons attributable to fat divided by all protons in the liver attributable to fat and water.
 Lola Koktysh, healthcare industry analyst at ScienceSoft.
Lola Koktysh, healthcare industry analyst at ScienceSoft.To separate the liver signal into its fat and water parts, chemical-shift imaging is applied. This technique acquires gradient echoes at appropriately spaced echo times. To increase examination accuracy, a low flip angle is used for minimizing T1 bias, along with multiple echoes for correcting T2* effects.
This approach suggests two alternatives. In one case, only the magnitude data are retained while the phase data are discarded. It allows users to accurately quantify the hepatic PDFF from 0% to 50%, which captures the biological range of human hepatic steatosis (rarely exceeding 50%).
Another alternative includes retaining both the phase and magnitude data and estimating the proton density fat fraction across the full dynamic range (0%-100%) of fat content in any tissue. Both options are reproducible across MR scanners and can be interpreted using medical image analysis software in clinical practice and trial.
The diagnostic accuracy of MRI-PDFF was validated by several studies, including Idilman et al and Bannas et al, which showed that MRI-based PDFF assessments closely correlated with histology acquired from liver biopsy.
MRS-based QIBs
Some researchers have suggested using MR spectroscopy for assessing PDFF, as it directly measures the differences in water and fat peaks on a resonance frequency domain. While it allows for higher accuracy in MRS-PDFF assessment, there are several limitations that require consideration.
Similar to liver biopsy, MRS data are collected from a single region or voxel positioned in the liver parenchyma. Thus, MRS algorithms quantify steatosis only within a small part of the liver, and they are unable to depict the full steatosis distribution throughout the liver parenchyma.
Then, the complexity of MRS examination requires substantial expertise on the part of the user to develop specific software for both acquisition and further medical image analysis. Moreover, MRS is not available on all MR scanners, which confines its routine adoption for clinical trials and clinical practice.
Last but not least, MRS is considered to be potentially more accurate; however, multiple studies (such as a September 2015 review in Mayo Clinic Proceedings) have shown that MRI-PDFF biomarkers have consistently been highly correlated with MRS-PDFF biomarkers in terms of diagnostic accuracy, reliability, and responsiveness.
Keeping in mind the ease of implementation, ability to quantify hepatic steatosis throughout the liver, and lack of additional expertise needed for image acquisition, MRI-based PDFF assessment proves to be a more suitable option for further clinical application than MRS-based assessment.
MRE-based QIBs
While MRI-PDFF is a promising biomarker for quantifying hepatic steatosis, its application for patients with more advanced liver disease is limited by the severity of fibrosis. To use MRI-PDFF for both diagnosing and evaluating treatment response in patients with more aggressive disease courses, MRE-based fibrosis quantification can be applied as an additional biomarker.
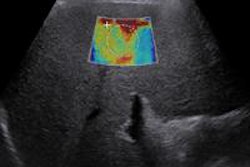
According to a November 2016 article in the Journal of Hepatology, MR elastography uses a modified phase-contrast pulse sequence to visualize rapidly propagating mechanical shear waves (typically delivered at around 60 Hz). Elastogram images depict the stiffness generated from the wave propagation information. It is even possible to enable MRE imaging with most MR scanners upon adding hardware to produce mechanical waves and add specific software for elastogram acquisition with algorithms for further processing. In this case, MRE examination can be carried out simultaneously with MRI.
Several studies have explored the diagnostic accuracy of MRE for quantifying hepatic fibrosis. For example, a study by Chen et al showed that MRE-based assessments of liver stiffness have high accuracy in differentiating NASH from simple steatosis, with a cutoff of 2.74 kPa yielding a sensitivity of 94% with a specificity of 73%.
Future of NASH QIBs
While MRI-PDFF and MRE can be reliable and noninvasive tools to assess hepatic steatosis and fibrosis, the implementation of these imaging modalities in both clinical practice and clinical trials has been limited. Multiple challenges are on the way -- from discussions on cost-effectiveness to technical feasibility and examination time required.
It is anticipated that a newer imaging modality that uses multiparametric MR imaging (T1 and T2* mapping) and proton spectroscopy could address some of the pitfalls. With this modality, medical images can be acquired in approximately 23 minutes using a conventional MRI scanner. Moreover, image analysis software could simultaneously assess steatosis and fibrosis on the scan, which would allow diagnosis to be streamlined and sped up.
However, further validation and technical refinement are still required for MRI-PDFF, MRE, and newer techniques to be commonly accepted as quantitative imaging biomarkers for detecting, grading, and treating NASH.
Lola Koktysh is a healthcare industry analyst at ScienceSoft, a custom software development company with 11 years of healthcare IT experience. ScienceSoft has a major focus on harnessing medical image analysis for automated diagnostics and quantitative imaging biomarkers for objective evaluation of patient conditions. More information is available on the company's website.
The comments and observations expressed herein are those of the author and do not necessarily reflect the opinions of AuntMinnie.com.