Shoulder MRI shows a high prevalence of accessory infraglenoid muscle (AIGM) in patients with teres minor fatty infiltration (TMFI), according to award-winning research presented May 6 at the American Roentgen Ray Society (ARRS) annual meeting.
In her online poster presentation, Jennifer Padwal, MD, from Stanford University Medical Center in Stanford, CA, demonstrated how TMFI in patients was mostly grade 1 or 2 as found by MRI.
“The presence of AIGM on shoulder MRI could negate the need for additional imaging to evaluate the cause of TMFI,” Padwal said.
TMFI has important prognostic implications for shoulder surgery, Padwal said. While quadrilateral space-occupying lesions, such as paralabral cysts or fibrous bands, are usually considered in assessing TMFI, the AIGM can be overlooked in evaluations and have negative effects on the axillary nerve. Padwal noted that the presence of TMFI on preoperative MRI is tied to poor postsurgical outcomes.
Previous research has shown a high prevalence of AIGM, but there is a lack of data comparing the prevalence of AIGM in patients with and without TMFI.
Padwal and colleagues performed an institutional review of all shoulder MRIs and included imaging data from 100 patients with documented TMFI. Of the total, 76 were men and 24 women, and the cohort had an average age of 58.6. For comparison, the team also included a respective sample of 100 shoulder MRIs in patients without TMFI. This included 53 men and 47 women with an average age of 56.4.
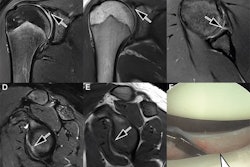
 Coronal MR images of a 66-year-old woman show definite small AIGM (blue arrows), corresponding to diagnostic confidence of 4. There is also high-grade glenohumeral osteoarthrosis, as well as small joint effusion (purple arrow).ARRS
Coronal MR images of a 66-year-old woman show definite small AIGM (blue arrows), corresponding to diagnostic confidence of 4. There is also high-grade glenohumeral osteoarthrosis, as well as small joint effusion (purple arrow).ARRS
Two radiologists performed consensus evaluations of MRI scans for an AIGM with diagnostic confidence. These included a musculoskeletal radiologist with 25 years of experience and a fourth-year radiology resident. They measured the distance between the AIGM and axillary nerve in patients with TMFI and from there, graded the TMFI cases.
The researchers found that TMFI was grade 1 in 33% of cases, grade 2 in 32% of cases, grade 3 in 13%, and grade 4 in 14%. This included 33 patients with intramuscular edema and 21 patients with atrophy.
The team also observed AIGM in 89 out of 100 patients with TMFI (89%) and 30 out of 100 patients without TMFI (30%).
In all cases, the AIGM originated from the inferior glenoid neck and inserted into the humeral neck/proximal humeral diaphysis. Finally, the inferior margin of the AIGM in patients with TMFI touched the axillary nerve in 39 patients (46%), with abnormal signal noted in 23 (27%) patients.
Padwal said that these findings highlight the importance of the importance of searching for AIGM in TMFI cases. The online poster was awarded ARRS Annual Meeting Magna Cum Laude honors.