In Europe, low-dose involved-field radiotherapy (IFRT) has been used for years as a palliative treatment for patients with non-Hodgkin's lymphoma due to a high patient response rate and minimal toxicity. Now, researchers in the U.S. are reporting similar findings.
Researchers at the Dana-Farber Cancer Institute in Boston evaluated treatment with low-dose IFRT in a group of 33 men and women with non-Hodgkin's lymphoma, the results of which were published in the Annals of Oncology (December 2008, Vol. 19:12, pp. 2043-2047).
Indolent, also called low-grade, non-Hodgkin's lymphoma is most often diagnosed at stage III/IV and is considered an incurable disease. Disease progression is typically characterized by multiple relapses with spontaneous remission. Even patients with an advanced stage of the disease can expect to live, on average, six to 10 years after diagnosis.
Because indolent lymphoma has a high level of radiosensitivity, local radiation therapy as well as chemotherapy can play an important role in achieving repeated remissions. However, conventional-dose radiation therapy often causes significant toxicity, including mucositis and xerostomia for head and neck treatments, gastrointestinal toxicity for abdominal treatments, and marrow toxicity with large pelvic fields. Delivering IFRT at a lower dose can minimize some of these effects.
In their study, the Dana-Farber researchers treated the 33 patients over a 50-month period commencing April 2004. None of the patients experienced any treatment toxicity, and response was very rapid for 31 patients.
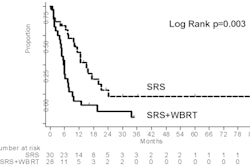
Eighty-four percent of the patients achieved a complete response, and 95% of the patients had an overall response, according to lead author Sarah Luthy, then a medical researcher at Dana-Farber, and Dr. Andrea Ng, associate professor of radiation oncology at Harvard Medical School in Boston. The follow-up period for the patient cohort ranged from one week to more than three years, with a median follow-up period of 14 months.
The patient group consisted of 14 women and 19 men, ranging in age from 28 to 75 years. Their median age at time of low-dose IFRT was 57. The time between diagnosis of non-Hodgkin's lymphoma and this treatment ranged from two months to more than 17 years, with a median interval of four years.
Prior to receiving low-dose IFRT, 52% of the patients had received systemic therapy, 45% had received conventional-dose radiotherapy, and 9% underwent stem cell transplants. Twenty-seven percent had received no prior treatment.
All patients received a total dose of 4 Gy delivered in two fractions over two consecutive days. The median size of the largest node of the 43 sites was 35 mm (range, 12-100 mm), and the anatomical sites treated included:
- Head and neck -- 21 treatments (49%)
- Pelvic and/or inguinofemoral nodes -- 11 treatments (26%)
- Cutaneous sites -- six treatments (14%)
- Axilla -- three treatments (7%)
- Peripheral node -- one treatment (1%)
- Breast -- one treatment (1%)
With this patient cohort, the researchers determined that the likelihood of achieving a complete response was significantly influenced by disease size. The finding of a significantly higher complete response rate for head and neck sites than for pelvic and/or inguinofemoral sites could be due to the difference in the sizes of the diseases in the two anatomical regions, the authors hypothesized. Neither age nor receipt of prior treatment was predictive of response to low-dose IFRT.
Fourteen patients have required no additional treatment. However, 19 patients had disease progression, and 16 patients required systemic therapy at a median time interval of eight months. Seven of the patients had their disease transfer to more aggressive histologies, and one of the patients died.
The use of low-dose IFRT allowed the delay of further systemic therapy by at least six to eight months for the majority of the patients, in addition to providing a high response rate with negligible toxicity.
Based on the results of the study and prior published European studies, the department of radiation oncology at Dana-Faber reserves conventional-dose radiation therapy (30-36 Gy) for patients with early-stage disease, for which the treatment intent is curative, and continues to use low-dose IFRT to provide palliative treatment.
By Cynthia E. Keen
AuntMinnie.com staff writer
February 11, 2009
Related Reading
Treatment-related AML and MDS rates 'acceptably low' after radiotherapy for NHL, October 5, 2007
Copyright © 2009 AuntMinnie.com