Kilovoltage and megavoltage conebeam CT are predominantly used for real-time imaging during radiation therapy, with systems based on ultrasound or MRI now also being developed. But there are other imaging modalities that could be used, including those that offer functional and molecular information regarding the tumor being treated.
At the recent American Association of Physicists in Medicine (AAPM) annual meeting in Charlotte, NC, researchers described a number of novel approaches to real-time radiotherapy image guidance.
High-speed SPECT
SPECT offers great potential for functional and molecular imaging of the target tumor, but unfortunately, SPECT scans can take 20 minutes or more and may offer poor image resolution. To address this limitation, a team at Duke University is developing a robotic multipinhole SPECT system that can perform onboard imaging in just four minutes.
The SPECT system comprises seven pods, each containing seven pinholes. The pods move relative to one another, and the entire 49-pinhole system can also be moved around the patient using robotic control. The geometry is such that the target region-of-interest falls within the field-of-view of all the pinholes, while the pinhole-to-region-of-interest distance can be varied to avoid collision with the patient. Faster imaging is achieved because the system concentrates on a limited region-of-interest, in this instance, a 7-cm-diameter sphere.
 |
| Schematic of the robotic multipinhole SPECT system. |
The researchers evaluated their design using computer simulations of the XCAT phantom containing 10 7-mm and seven 10-mm in diameter spherical contrast inserts (with 6-to-1 radiotracer uptake). Simulations of images recorded by a conventional parallel-hole-collimated SPECT detector (also using four-minute scans) were used for comparison. Showing an example four-minute multipinhole image, James Bowsher, PhD, a medical physicist and assistant professor of radiation oncology, noted that all 10-mm spheres and all 7-mm spheres were apparent. Results for the reference parallel-hole detector were not nearly as good.
 |
| Simulated phantom images recorded by the multipinhole SPECT system and a conventional parallel-hole-collimated SPECT detector. |
In a numerical observer study, the multipinhole SPECT also performed better in localizing the hotspots than the parallel-hole system. Across an ensemble of 25 four-minute scans, localization was almost always better than 2 mm for the 10-mm spheres, with most results being better than 1 mm. For the 7-mm spheres, the multipinhole system also generally demonstrated better than 2-mm localization. Again, results were not nearly as good for the parallel-hole system.
"The multipinhole SPECT system design could perform imaging while a patient is in position for radiotherapy," Bowsher concluded. "It could improve region-of-interest imaging as compared to conventional parallel-hole-collimated, full cross-section SPECT."
Cerenkov radiation
Colin Carpenter, PhD, a postdoctoral research fellow in radiation oncology at Stanford University School of Medicine, described the use of Cerenkov imaging for real-time metabolic guidance of surgery or intraoperative radiotherapy. "We are developing a Cerenkov-based tool that will allow the surgeon or radiation oncologist to identify tumor areas that uptake contrast agent such as [the PET tracer] FDG," he explained.
Cerenkov radiation is emitted when a charged particle (emitted by decay of the FDG in this case) passes through a dielectric medium at a speed greater than the speed of light in that medium. Cerenkov imaging can potentially provide higher spatial resolution than PET and SPECT, but imaging Cerenkov photons can be challenging, due to the low-intensity signal produced.
The Stanford team built a customized Cerenkov imaging system based on an image-intensified CCD, which proved sensitive at Cerenkov wavelengths. Fiber-based optics maximize the light collection angle and also enable endoscopic imaging. They performed sensitivity tests using a 96-well plate, with one well filled with FDG and one with water. The imaging system detected Cerenkov radiation from the decaying FDG (and a background signal from the water) with a sensitivity of 1 µCi, roughly equivalent to FDG uptake in 1 mL of tissue.
The researchers then tested the imaging system's resolution using a commercial SPECT phantom containing cylindrical holes filled with FDG. "We can easily see the 1.6-mm holes in the phantom," said Carpenter. "The 1.2-mm holes were harder to see, but by optimizing the system, we think we can drive this lower to a resolution of less than 1 mm."
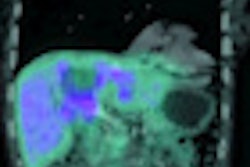
 |
| Cerenkov imaging of a glioma xenograft tumor using a commercial IVIS optical imaging system (A) and using the new customized imaging system (B). |
Finally, the team examined a mouse model with a subcutaneous tumor and FDG injected into the tail vein. Tumor tissue exhibited significantly higher Cerenkov optical emission than the healthy tissue. When the tumor was resected, the Cerenkov signal remained in the excised tumor. They also studied an invasive mouse prostate tumor model with metastases at unknown locations. Cerenkov imaging was used to guide resection, and areas with signal enhancement were excised. When the imaging was compared to subsequent pathology, they found a significant difference in uptake between tumor and healthy tissues.
Carpenter noted that this Cerenkov-based method could also be used to provide feedback during intraoperative radiotherapy, minimizing irradiation of normal tissue in the surgical cavity.
Emission guidance
A different take on molecular imaging for guiding radiotherapy was described by Sam Mazin, PhD, president of RefleXion Medical. PET offers high specificity and sensitivity across many cancers but is limited by the biotracer signal, requiring several minutes for enough events to occur to form a useable image.
Mazin and coworkers came up with the novel concept of using PET emission directly for real-time targeting, in a technique dubbed emission-guided radiation therapy (EGRT). EGRT exploits the fact that each detected pair of annihilation photons provides a direct line of sight to the emission source. After checking that the line of response intersects the planned target volume and that the detections occur within the correct time window, radiation is then delivered along this path.
In the proposed EGRT geometry, the two PET detectors are mounted on a rotating gantry along with the radiation source, enabling irradiation along each line of response as it is detected. Having previously demonstrated EGRT in phantoms, Mazin told the AAPM delegates about the first clinical feasibility study on a lung cancer patient (performed in collaboration with the Stanford Cancer Institute).
 Geometry of the emission-guided radiation therapy system.
Geometry of the emission-guided radiation therapy system.
The researchers used the patient's PET planning data as input to simulate the EGRT system's response in terms of multileaf collimator settings. They then employed Monte Carlo simulations to calculate the dose delivered to the patient. EGRT dosimetry results were compared with those from intensity-modulated radiotherapy (IMRT) of the same patient.
EGRT provided a higher dose to the gross tumor volume (GTV) than IMRT (18% relative increase in dose to 95% of the GTV), with the same lung V20 (volume receiving at least 20 Gy). This advantage was also seen when an integrated boost -- in which radiation beams intersecting a boost volume were weighted -- was included in the treatment. The researchers now plan to study EGRT's ability to target multiple tumors simultaneously, as well as perform biological dose adaptation, said Mazin.
© IOP Publishing Limited. Republished with permission from medicalphysicsweb, a community website covering fundamental research and emerging technologies in medical imaging and radiation therapy.