Sprained ankles would seem to be part and parcel of childhood. But when a simple sprain balloons into a serious problem -- characterized by swelling, bone tenderness, and even an inability to walk -- clinicians may be hard-pressed to come to a definitive diagnosis. While a three-view x-ray may reveal nothing out of the ordinary, an ultrasound exam can be very helpful.
"When (x-ray) is negative, the physician is faced with a discrepancy between the clinical and radiological data, yet a decision must be made.... A missed fracture can lead to inadequate treatment, causing prolonged pain and delayed ambulation," wrote Dr. Natalia Simanovsky and colleagues, who conducted a prospective study on the sonographic evaluation of radiographically negative ankle injuries in a pediatric population (Pediatric Radiology, November 2005, Vol. 35:11, pp. 1062-1065).
Simanvosky's group is from the departments of radiology and orthopedic surgery at Hadassah University Hospital in Jerusalem.
The study included 20 children with a mean age of 10 years. All were suspected of having a fracture despite a negative x-ray based on a joint assessment of the films by an orthopedic surgeon and a radiologist. A pediatric radiologist performed an ultrasound exam, in multiple longitudinal planes around the ankle, using a 5- to 12-MHz transducer (HDI 5000, Philips Medical Systems, Andover, MA).
Some of the ultrasound findings included ligamentous injury and the presence of fluid. Cases in which both sonographic results and follow-up x-rays (two to three weeks later) demonstrated a fracture were considered true-positive.
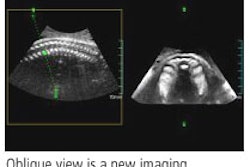
According to the results, ultrasound identified small metaphyseal cortical fractures of the distal fibula in five patients. Discontinuity of the echogenic cortical line and cortical depression were two of the sonographic hallmarks of fracture. In a sixth patient, a subcortical echogenic line was detected in the fibular metaphysis. In all six cases, local periosteal reaction was seen on the follow-up x-ray. The children were treated with a short walking cast and healed completely.
In the remaining 14 patients, no bone pathology was found with ultrasound. All follow-up x-rays were negative for periosteal reaction and fracture lines. They also successfully completed treatment.
"Possible reasons for nonvisualization of ankle fractures on radiographs include small size, nondisplaced fracture, and beam direction tangential to the cortical surface," the authors explained. "Based on these data, it could be suggested that a high number of fractures are underdiagnosed and treated as simple ankle sprain."
In addition to its diagnostic capability, ultrasound is noninvasive, less expensive, fast, and readily available, they concluded. For now, they recommended that it be used as an adjunct to x-ray, although it may serve as a replacement one day. A previous study determined that ultrasound can reduce the number of x-rays needed for diagnosing long bone fractures and could serve as the primary imaging modality (Journal of Bone and Joint Surgery British, November 2000, Vol. 82:8, pp. 1170-1173).
By Shalmali Pal
AuntMinnie.com staff writer
January 23, 2006
Related Reading
MRI can't replace x-ray for pediatric growth plate injuries, December 1, 2005
Ankle cartilage MRI improved by force, November 28, 2005
Tibial-talar ratio on x-ray reliably shows ankle alignment, May 6, 2005
Copyright © 2006 AuntMinnie.com