Performing bedside ultrasound on emergency department (ED) patients with undifferentiated hypotension can reduce diagnostic uncertainty and have a clinically significant impact on more than half of cases, according to research from George Washington University (GWU) Medical Center.
In addition, the prospective study also found that bedside ultrasound could have a dramatic impact on the management of a small number of patients.
"A hypotension protocol is an optimal use of point-of-care ED ultrasound that exemplifies 'right time, right place,' " said Dr. Hamid Shokoohi of the GWU Department of Emergency Medicine.
Undifferentiated hypotension is a critical ED presentation, and patient management is directed toward narrowing the differential diagnosis. With early goal-directed therapy considered essential for an optimal outcome, bedside ultrasound has been proposed as a means to rapidly stratify competing diagnoses, according to Shokoohi.
Shokoohi presented his research findings during a presentation at the American Institute of Ultrasound in Medicine (AIUM) annual meeting earlier this year.
Aiming to validate previous studies exploring the use of ultrasound on ED patients with undifferentiated hypotension, the study team set out to assess a bedside ultrasound protocol on management, examining its impact on improvement in diagnostic certainty, its ability to identify definitive and unexpected findings, and the concordance between ultrasound findings and final diagnosis.
The GWU researchers prospectively evaluated a convenience sample of 72 patients at GWU Medical Center with undifferentiated hypotension. All patients were more than 18 years old and had systolic blood pressure less than 90 mm Hg and no known source of hypotension.
Emergency medicine attending physicians were surveyed after an initial clinical evaluation of the patient, and goal-directed ultrasound was then performed using a M-Turbo compact-ultrasound scanner (SonoSite) by credentialed emergency sonologists not directly involved with patient care.
A standard ultrasound protocol for hypotension was employed, including a cardiac study (encompassing ejection fraction estimation, right ventricular [RV] dilation, and the presence or absence of pericardial effusion and tamponade), inferior vena cava (IVC) diameter measurement, a FAST (focused assessment with sonography for trauma) exam, an aorta scan (to check for abdominal aortic aneurysm), and a thoracic study (to detect pneumothorax).
After receiving the ultrasound results, the emergency medicine attending who evaluated the patient was surveyed again. The pre- and post-test questionnaire given to the attendings included a certainty matrix for estimated diagnostic certainty in six categories of hypotension etiologies: sepsis, cardiogenic, pericardial effusion, pulmonary embolism, hypovolemia/bleeding, and other. Certainty range choices included 0% to 25%, 25% to 50%, 50% to 75%, and 75% to 100%.
Physicians were also asked questions on how ultrasound affected management parameters, the need for further testing, the need for consultations in the ED, and how ultrasound changed the disposition of the patient in the ED.
The researchers have focused their initial data analysis on the main outcome of measuring the impact of the ultrasound protocol on the attending's diagnostic certainty. Using a tool to quantify diagnostic uncertainty derived from Shannon Information Theory, this method quantifies uncertainty by creating a summation score of diagnosis, with each diagnosis in the differential treated as a "bit" of information, Shokoohi said.
Changes in the summation scores were noted before and after the ultrasound protocol. Decreased uncertainty was interpreted as enhanced decision-making in diagnosis and treatment.
Bedside ultrasound reduced diagnostic uncertainty (as measured by the summation scores) from a mean of 1.77 to 1.51 (95% confidence interval [CI]: -0.13 to -0.38). The difference was statistically significant.
In 37 (51%) of 72 patients, ultrasound had a clinically significant impact, as determined by two or more quartile changes in physicians' perception of likelihood of diagnosis following ultrasound. Ultrasound also led to a significant increase in the absolute proportion of patients with a definitive diagnosis, climbing from 5.6% to 16.7% [95% CI: 1.0% to 21.2%].
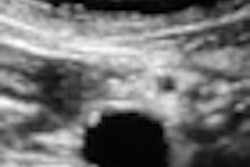
 A 26-year-old woman with upper abdominal pain, chest pain, and no history of trauma. She presented to the ED with hypotension after watching a golf game and required CPR shortly after triage in the ED. First impression was ruptured ectopic pregnancy versus pulmonary embolism, but ultrasound revealed a ruptured splenic artery aneurysm. Images courtesy of Dr. Hamid Shokoohi.
A 26-year-old woman with upper abdominal pain, chest pain, and no history of trauma. She presented to the ED with hypotension after watching a golf game and required CPR shortly after triage in the ED. First impression was ruptured ectopic pregnancy versus pulmonary embolism, but ultrasound revealed a ruptured splenic artery aneurysm. Images courtesy of Dr. Hamid Shokoohi.
In other findings, Shokoohi reported that ultrasound found abnormal IVC diameter in 46% of patients, abnormal ejection fraction in 36%, RV dilation in 14%, peritoneal and pleural free fluid in 13%, pericardial effusion in 8%, tamponade in 1.4%, and abdominal aortic aneurysm in 1.4%. No pneumothorax cases were found.
While ultrasound did not have a clinically significant impact in 49% of patients, Shokoohi noted that in a small number of cases, ultrasound yielded dramatic changes in diagnosis and management.
"In this minority of cases, you find the diagnosis [with ultrasound] that none of us can afford to miss," Shokoohi said.