Adding shear-wave elastography to a second-look breast ultrasound study performed after dynamic contrast-enhanced MRI (DCE-MRI) can detect nearly a third more cancers than B-mode ultrasound alone, Ohio researchers have found.
In a prospective study of 73 women, shear-wave elastography increased cancer detection during second-look ultrasound by 31%. Furthermore, shear-wave elastography yielded a high negative predictive value, increasing confidence that findings will have concordance with pathology, said Dr. Donna Plecha, director of breast imaging at University Hospitals Case Medical Center in Cleveland. Plecha presented the research during a session at the recent American Roentgen Ray Society (ARRS) annual meeting.
"Real-time [shear-wave elastography] added to routine B-mode ultrasound scanning may help confidently detect subtle cancers, increasing the number of cancers detected during second-look ultrasound after DCE-MRI," Plecha told AuntMinnie.com.
Detecting more lesions
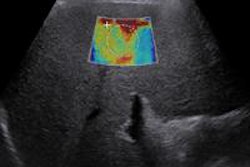
Performed after DCE-MRI, second-look ultrasound provides visualization of lesions and allows for immediate ultrasound-guided biopsy. A highly reproducible technique, shear-wave elastography evaluates stiffness by measuring propagation shear waves within tissue, according to the researchers. It can be used while moving the ultrasound transducer over the breast and searching for a lesion.
To see if adding shear-wave elastography to a second-look breast ultrasound study could improve the detection and characterization of lesions, the researchers enrolled 73 women (median age, 52 years; range, 21-84) between May 2011 and August 2012. All patients received shear-wave elastography during their second-look ultrasound after one or more lesions were found on DCE-MRI.
MRI studies were performed on either a Magnetom Avanto or Magnetom Espree 1.5-tesla scanner (Siemens Healthcare) using a dedicated breast coil. All lesions that were BI-RADS category 4 and 5 after DCE-MRI were evaluated using second-look ultrasound, and both B-mode ultrasound and shear-wave elastography were performed using an Aixplorer ultrasound system (SuperSonic Imagine) with a 12-5 MHz linear-array transducer.
Patients were initially scanned with B-mode ultrasound. If B-mode ultrasound correlated with the MRI-detected lesion, then shear-wave elastography was employed to map tissue stiffness. In the event that B-mode ultrasound did not reveal a definite lesion, one of five fellowship-trained breast radiologists scanned with shear-wave elastography in real-time to look for areas of stiffness, find isoechoic or subtle lesions, and confirm questionable lesions, according to the researchers.
Qualitative color shear-wave elastographic stiffness was evaluated for all lesions using a five-point color score of maximum elasticity in the mass and surrounding parenchyma, according to the researchers.
All 96 lesions received ultrasound-guided or MRI-guided core biopsy, and the researchers recorded pathology results for all lesions. Of the 96 lesions, 28 (29%) were malignancies, 14 (14%) were high-risk lesions, and 55 (57%) were benign lesions.
High sensitivity, specificity
Grouping elastography findings into softer lesions (elastography color scale of 1 or 2) and stiffer lesions (elastography color scale of 3, 4, and 5), shear-wave elastography had sensitivity of 95.2%, specificity of 70%, positive predictive value of 71.4%, and negative predictive value of 91%.
| Cancer detection by modality | ||
| Modality | Cancer cases | % of total cancers (n = 28) |
| MRI only | 7 | 25% |
| B-mode ultrasound only | 16 | 57% |
| B-mode ultrasound and shear-wave elastography | 21 | 75% |
Lesions seen on second-look ultrasound were more likely to be cancer than lesions seen only on MRI (p = 0.006). Shear-wave elastography found five of the 50 lesions seen on second-look ultrasound, and all five were invasive cancer. Four were invasive ductal carcinoma and one was an invasive lobular carcinoma.
Of the lesions found with DCE-MRI, 84 (87%) were masses; 48 (57%) were also found on second-look ultrasound, avoiding the need for MRI biopsy. The remaining 12 (13%) were nonmass enhancements, and two (17%) of these were found on ultrasound. Ultrasound was significantly more likely to find mass enhancement (p = 0.012).
"Ultrasound-guided biopsy of DCE-MRI BI-RADS category 4 or 5 lesions remains preferable to MRI biopsy because of its relative ease, lower cost, and improved patient comfort," Plecha told AuntMinnie.com. "The high negative predictive value of the five-point color score of maximum elasticity may help with the confidence level of the radiologist when correlating a benign biopsy result with the B-mode ultrasound image."
In the next phase of research, the group plans to include more patients to try to increase statistical significance, Plecha said.