
Very few incidentally detected thyroid cancers would be missed if recommendations from the Society of Radiologists in Ultrasound (SRU) for thyroid nodules were followed. What's more, the nodules not worked up are unlikely to become a problem, according to research published in the June issue of Radiology.
In a retrospective 10-year review, a team led by Dr. Manisha Bahl from Duke University Medical Center found that adopting SRU guidelines for follow-up of incidental thyroid nodules would result in only 2% of thyroid cancers being missed. In addition, the missed tumors tended to be much smaller and more likely to be stage I than those found during workup recommended by the SRU guidelines.
"When the SRU criteria-negative incidental cancers are compared to SRU criteria-positive incidental cancers, they are smaller in size, more likely to be papillary carcinoma, and less likely to have nodal metastases," senior author Dr. Jenny Hoang told AuntMinnie.com. "In general, these characteristics belong to thyroid cancers that are more likely to have an indolent course and may never become symptomatic in the patient's lifetime."
A big problem
Incidental thyroid nodules spotted on ultrasound and other imaging modalities are a big healthcare problem in the U.S.: The nodules are common and workup can lead to patient anxiety and unnecessary and costly procedures or surgery, Hoang said.
Guidelines such as SRU's thyroid recommendations are important in reducing the growing number of biopsies being performed for incidental thyroid nodules. However, the SRU recommendations -- which were published in 2005 -- have not been widely adopted by clinicians and radiologists, including those at Duke, she said.
A previous Duke study found that using SRU recommendations could prevent 30% of biopsies. However, that study population consisted mostly of benign nodules "and did not adequately address the fear of missing more cancers in a larger cohort of patients with incidental thyroid nodules over time," she said. "In this paper we specifically addressed that fear: How many incidental cancers would be missed with the SRU recommendations over a decade?"
The group retrospectively reviewed data from thyroid surgery patients from January 1, 2003, through December 31, 2012. After evaluating imaging studies and reports for incidental thyroid nodules, the team categorized incidental nodules using the SRU criteria to ascertain the characteristics of malignant nodules that would and would not have been worked up (Radiology, June 2014, Vol. 271:3, pp. 888-894).
Of the 2,090 thyroid surgery patients included in the study, 680 were found to have thyroid cancer; 101 (15%) had incidental thyroid nodules detected on imaging. After the researchers applied the SRU recommendations to the 90 patients who had available ultrasound images or reports, they determined that 16 (18% of the 90 patients and 2% of all thyroid cancers) would have been missed using the criteria.
The tumors that would not have been worked up under the SRU criteria had a mean size of 1.1 cm (range, 0.9-1.4 cm), compared with a mean size of 2.5 cm (range, 1.0-7.6 cm) for those that had met the SRU recommendations. The difference was statistically significant (p < 0.001). Nearly all (15/16, 94%) were stage I, compared with 47 (64%) of the 74 incidental thyroid nodules that met the SRU criteria.
Fourteen (88%) of the 16 SRU criteria-negative cancers were papillary carcinoma; small papillary carcinoma has an extremely high survival rate. The other cases were a follicular carcinoma and a medullary carcinoma.
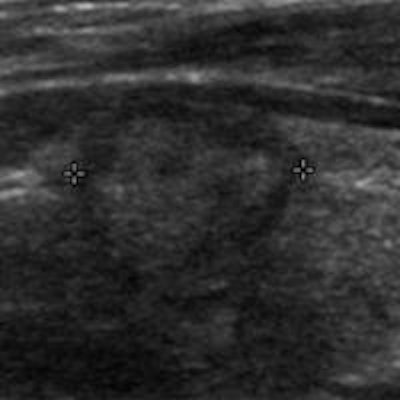
 Transverse ultrasound image of an SRU criteria-negative thyroid cancer. Incidentally detected at CT, this 1.2-cm thyroid nodule is solid in composition. It does not meet the SRU recommendations for fine-needle aspiration biopsy. The postsurgical pathologic result was papillary cancer. Image courtesy of Dr. Manisha Bahl.
Transverse ultrasound image of an SRU criteria-negative thyroid cancer. Incidentally detected at CT, this 1.2-cm thyroid nodule is solid in composition. It does not meet the SRU recommendations for fine-needle aspiration biopsy. The postsurgical pathologic result was papillary cancer. Image courtesy of Dr. Manisha Bahl.The researchers were surprised to find that patients with incidental thyroid cancers only represented 15% of patients who had surgery for thyroid cancer, Hoang said. The group's two prior studies had found that 29% of patients with incidental thyroid nodules underwent ultrasound-guided biopsy and 23% of patients had thyroid surgery for nodules.
"The overall lower proportion of incidental thyroid cancers among all thyroid cancer patients simply highlights the fact that benign incidental thyroid nodules are common, but cancer among the incidental nodules is uncommon," she said.
For practicing radiologists and clinicians, the clinical implication from this study and the group's prior studies is that SRU recommendations "can be used to better manage workup of incidental thyroid nodules and that SRU recommendations achieve the goal of ensuring that clinically important thyroid cancers would undergo biopsy, while avoiding unnecessary tests and surgery in patients with benign nodules," Hoang said.
Adoption of guidelines
In addition to SRU, the American Association of Clinical Endocrinologists (AACE) and the American Thyroid Association (ATA) have guidelines that recommend fine-needle aspiration (FNA) biopsy of thyroid nodules based on ultrasound findings. When speaking with a number of radiologists from different practice types over the past couple years, Hoang was most commonly told that the clinician decides which nodules receive biopsies.
"Most clinicians use a size cutoff of 1 cm for solid nodules which is part of the AACE and ATA guidelines," she said. "This is seemingly a small difference compared to the SRU 1.5-cm cutoff [for nodules without microcalcification], but another study from our group showed that one in four biopsies could be prevented with the SRU recommendations. Therefore, increasing the size cutoff by just 5 mm can substantially reduce the proportion of thyroid nodules that require biopsy."
Hoang said that she hopes this study will encourage more widespread adoption of the SRU recommendations.
"Radiologists and clinicians now have our study to allay fears of missing many and significant cancers by being more selective in the workup of incidental thyroid nodules," she said.
Hoang also noted that she is a member of an American College of Radiology (ACR) committee that will produce a white paper in the coming year on incidental thyroid nodules for all imaging modalities. Furthermore, Duke has developed a three-tier system for reporting incidental thyroid nodules found on CT, MRI, or PET/CT, she said.

















