
In a case report from Texas, echocardiography helped clinicians diagnose a man with a rare case of infective endocarditis (IE) thought to be caused by oral bacteria released from vigorous dental flossing. The findings were published in the Cureus Journal of Medical Science.
A transesophageal echocardiogram of the man revealed vegetation, an infected mass growing on a heart valve that is a hallmark of infective endocarditis. This is believed to be the first known case of the disease stemming from robust flossing, according to the authors.
"No previous case has been described with flossing-induced IE on a native mitral valve," wrote the group, led by Dr. Rachel Bridwell from Brooke Army Medical Center at Fort Sam Houston in San Antonio.
An elusive disease
Infective endocarditis is a rare disease in which a bacterial infection can lead to inflammation and damage to the heart valves. Early diagnosis is critical, as the condition has a mortality rate of 10% to 30%. IE is challenging to diagnose due to its various subtle presentations and underlying risk factors, including use of intravenous drugs, having an implantable cardiac device, undergoing recent dental work, or being immunocompromised.
Native mitral valve IE, which was the man's diagnosis, represents a small but important subset of the disease. The mitral valve does not experience the same high pressures and later rates of calcification as the aortic valve; however, chronic regurgitation and prolapse of the two-leaflet structure wears the valve and makes it more inclined to grow vegetation, the authors wrote.
Prior evidence has shown that flossing may protect against infective endocarditis. This case is unique because forceful flossing is believed to have led to colonization with the bacteria Streptococcus gordonii, causing this patient's infective endocarditis.
63-year-old man
A 63-year-old man with a medical history of mitral regurgitation went to the emergency room because he had a fever of 103° F for three weeks. Previously, he had been evaluated at another emergency department and by a primary care doctor for the same reason, but the fever persisted without a known cause. He denied having any risk factors, including recent dental work and drug or alcohol use. However, the man endorsed robust flossing that caused his gums to bleed, the authors noted.
His vital signs were normal, an exam did not identify a murmur or skin lesions, and an electrocardiogram and chest x-ray did not show any abnormalities. His lab results revealed a white blood cell count of 10,100 cells/uL, an elevated C-reactive protein level of 14 mg/dL, and an erythrocyte sedimentation rate of 95 mm/h. The man was given 1.5 g of vancomycin and 3.375 g of piperacillin/tazobactam intravenously.
Three separate blood cultures collected 15 minutes apart yielded S. gordonii. A transthoracic echocardiogram (TTE) didn't show anything remarkable, but a transesophageal echocardiogram (TEE) revealed a small vegetation on the posterior leaflet of the mitral valve. His antibiotics were changed to 242 mg of intravenous gentamicin every 24 hours and 24 million units of penicillin G continuous infusion, due to the sensitivities of S. gordonii, the authors wrote.
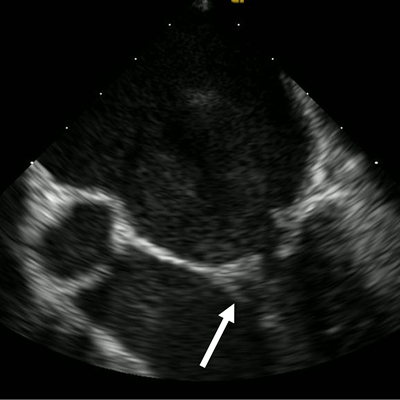
 The transesophageal echocardiogram shows a small, independently mobile linear echodensity on the posterior leaflet of the mitral valve (white arrow). This is consistent with vegetation. Image courtesy of Bridwell et al. Licensed under CC BY-NC 4.0.
The transesophageal echocardiogram shows a small, independently mobile linear echodensity on the posterior leaflet of the mitral valve (white arrow). This is consistent with vegetation. Image courtesy of Bridwell et al. Licensed under CC BY-NC 4.0.The man's blood cultures no longer grew S. gordonii on his third day in the hospital. He was discharged home and prescribed two weeks of outpatient gentamicin infusions and four weeks of penicillin infusions.
Lessons learned
Once a patient is admitted to the hospital for suspected infective endocarditis, he or she should receive antibiotics along with comprehensive TEE and TTE. These imaging modalities can identify 90% of all vegetations when they are performed within 12 hours of hospital admission, according to the authors.
Emergency physicians should consider this diagnosis in patients with high-risk features, such as recent dental work, and recurrent fevers without an identified source, they concluded.
"While toothbrushing in a patient with poor dental hygiene has been estimated to increase bacteremia risks far more than a single tooth extraction, there are no data to suggest the same incurred risk for flossing," the authors wrote. "In fact, flossing has been associated with a decreased risk of IE, highlighting the unique nature of this case."



















