When using ultrasound to follow up on suspicious breast masses in patients who just got a second dose of a COVID-19 vaccine, it may be wise to postpone scans to between 12 and 16 weeks to reduce unnecessary biopsies, according to research published December 22 in the American Journal of Roentgenology.
A team led by Dr. Derek Nguyen from Johns Hopkins University in Baltimore found that patients who were not recommended for biopsy had a median interval of 15.9 weeks between the second vaccine dose and ultrasound follow-up. This suggests that the amount of time needed for adenopathy-related reactions to the vaccines to subside is greater than 12 weeks.
"To our knowledge, this study represents the largest published cohort to date to evaluate histopathology of suspected COVID-19 vaccine-related axillary adenopathy," Nguyen and colleagues said.
Adenopathy that's visible on breast screening exams is a known side effect of COVID-19 vaccination. The Society of Breast Imaging recommends short-term follow-up breast examination at four to 12 weeks for patients with unilateral axillary adenopathy after they receive the second dose of the COVID-19 vaccine.
Biopsy may be considered if adenopathy persists at follow-up. However, unnecessary interventions may occur if patients return early within the follow-up range. Therefore, Nguyen et al wanted to study the ultrasound characteristics and histopathology of COVID-19 vaccine-related axillary adenopathy.
The team looked at data from 94 women between December 2020 and August 2021 with an average age of 56 years, 32 of whom underwent biopsy. The women were given a BI-RADS category of 3, 4, or 5 for assessment of unilateral adenopathy.
The median interval between the second vaccine dose and decision to biopsy was 15 weeks. Researchers found that women who received a biopsy recommendation had a shorter median time interval between the second vaccine dose and decision to biopsy at 12.9 weeks, compared with women who did not receive biopsy recommendation at an average of 15.9 weeks (p = 0.04).
Women who received a biopsy recommendation more commonly underwent axillary ultrasound within 13 weeks of the second vaccine dose at 50% than women who didn't receive such recommendation at 27% (p = 0.03).
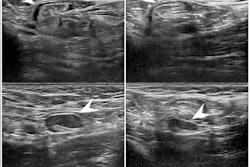
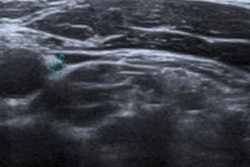
The median maximal cortical thickness on initial ultrasound was found to be 5 mm in women who were recommended biopsy, compared with 4 mm for women who weren't recommended.
Three patients were diagnosed with malignant axillary adenopathy. Biopsy was recommended for all three from 12 to 13.1 weeks after the second vaccine dose. They also had a maximal cortical thickness of at least 5 mm and "highly suspicious" sonographic features, the researchers said.
The opposite could be said for all 29 women who had benign biopsy. They had symmetric cortical thickening and no suspicious sonographic features.
Ten of the total number of women who had biopsy performed on them were recommended more than 12 weeks after the second vaccine dose, all of whom had benign pathology results.
The researchers called for revising current management guidelines for COVID-19 vaccine-related axillary adenopathy to promote more standardized evidence-based clinical practice.
"Further, regardless of vaccine dose timing, a low threshold for biopsy should be considered for unilateral axillary adenopathy with highly suspicious sonographic findings, to not delay cancer diagnosis," the study authors wrote.