
Classifying lesions found on ultrasound through the Thyroid Imaging Reporting and Data System (TI-RADS) is beneficial, but improvements can be made, according to research presented May 3 at the American Roentgen Ray Society (ARRS) meeting in New Orleans.
Researchers in three separate but related presentations discussed existing and new research that shows the effectiveness of TI-RADS in thyroid imaging with ultrasound.
"It provides descriptive features that are associated with increased rates of malignancy," said Dr. Michelle Melany from Cedars-Sinai Medical Center in Los Angeles in her keynote speech. "It helps categorize nodules and increases the number of reports with unambiguous management recommendations."
The American College of Radiology (ACR) in 2017 developed a standardized TI-RADS risk-stratification system to inform practitioners about which thyroid nodules require biopsy. This was in response to costly interventions for nodules that turned out to be benign on biopsy.
TI-RADS uses a scoring scale that goes from 0 to 5. A score of 0 indicates a benign lesion, while 5 represents a highly suspicious finding.
Benefits of TI-RADS include having higher sensitivity than risk stratification systems, ensuring all nodules can be classified, and reducing unnecessary biopsies, among others.
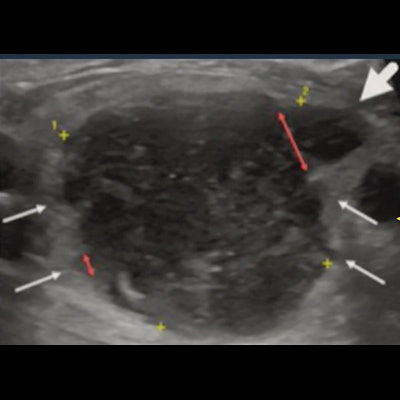
 The Thyroid Imaging Reporting and Data System (TI-RADS) has been used as a standardized method for classifying thyroid nodules. It was introduced by the American College of Radiology in 2017, but researchers at the 2022 ARRS meeting presented abstracts showing the system can be improved. This image from researchers at the Mayo Clinic in Arizona shows macro- and microlobulations on thyroid ultrasound.
The Thyroid Imaging Reporting and Data System (TI-RADS) has been used as a standardized method for classifying thyroid nodules. It was introduced by the American College of Radiology in 2017, but researchers at the 2022 ARRS meeting presented abstracts showing the system can be improved. This image from researchers at the Mayo Clinic in Arizona shows macro- and microlobulations on thyroid ultrasound.However, in her ARRS 2022 talk, Melany also listed some challenges the system faces. These include having a higher interobserver variability, varying appearances, and dependence on scanning parameters.
"In most of our practices, we're super busy. If only the ultrasound technician scans, then we're really dependent on what's captured and recorded on still images or cinematic clips," Melany said.
In an abstract presentation following Melany's keynote address, Dr. Logan Haug from the Mayo Clinic in Arizona showed research he co-led assessing whether adjusting TI-RADS could further reduce including benign nodules while keeping all malignant nodules. The current TI-RADS assign a score of two points for any lobulation found on ultrasound.
The team retrospectively looked at all ultrasound and pathology records to identify 516 thyroid nodules that underwent fine-needle aspiration (FNA) and had 58 lobulated margins in a two-year period. Images were divided into two groups showing "only macrolobulated" or "microlobulations present." Microlobulations were defined as being less than 2.5 mm in circumference.
Out of the lobulated margins, 14 were found to be malignant. A total of 37 lobulated margins were solely macrolobulated (two malignant), while 21 were microlobulated (12 malignant) (p < 0.0001).
Of nodules greater than or equal to 10 mm, 53 were lobulated, including 10 malignancies. The researchers found that under current TI-RADS standards, all 53 nodules met the criteria for FNA. However, under the team's microlobulation TI-RADS standards, 38 met the criteria for FNA
In a second abstract presentation, Dr. Meredith Bara from the University of Alberta in Canada talked about research she co-led that looked at interreader agreement after teaching sessions for residents.
The study authors used 50 test nodules scored independently by three radiology residents with no formal TI-RADS training. Bara said the residents underwent a one-hour teaching session after initial scoring, which included reviewing sonographic features of nodules and 30 training cases.
The team found that the residents showed "significant" improvement in agreement after training, with a pooled specificity between 76.6% and 96.8%. They showed the strongest agreement on nodular shape and composition.
Melany in her keynote listed some potential future modifications to TI-RADS that could further improve its effects. These include using active surveillance, changing points for certain features, incorporating nodule location, using artificial intelligence, and using newer ultrasonic methods such as contrast-enhanced ultrasound and elastography.

















