_20210915221258.png?auto=format%2Ccompress&q=70&w=400)
Clinicians in Japan successfully performed a temporomandibular joint (TMJ) ankylosis surgery on a pediatric patient using a computer-assisted navigation system, according to details published on September 10 in the Journal of Medical Case Reports.
Employing an electromagnetic navigation system to avoid damage to the young patient's brain, the clinicians made a preauricular incision and then performed an interpositional gap arthroplasty using temporal muscle and fascia as the interpositional graft materials.
"A navigation system is helpful for confirming the exact target locations and ensuring safe surgery," wrote the group, led by Ryo Miyazaki of the department of oral and maxillofacial surgery at Kagawa University.
TMJ surgery using the navigation system
In 2012, the 7-year-old girl was referred to the hospital with trouble opening her mouth. She had a facial bruise after falling from a pull-up bar two years earlier in August 2010. During that first visit, she had severely limited motion of her right mandible, and her maximum oral aperture was 13 mm.
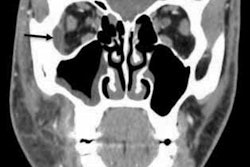
Prior to the surgery, the patient underwent panoramic radiography and CT scans that showed a deformity of the left condyle caused by bone addition as well as a loss of joint space. The joint cavity and articular disk were not visible on MRI.
The clinical team used an electromagnetic navigation system -- a Medtronic StealthStation S7 workstation with Synergy Fusion Cranial software -- to measure the girl's skull and confirm the position of the medial cranial fossa and the distance from the glenoid fossa to the skull base.
They set a reference point on the patient's forehead, placed a magnetic field generator on the side of her head, and performed registration with the tracer probe.
.png?auto=format%2Ccompress&dpr=2&fit=max&q=70&w=700) Above: Intraoperative photos demonstrating a bony fusion between the condylar head and glenoid fossa (A), the use of the navigation system to confirm the operating position (B), the formed articular cavity (C), and the temporal muscle insertion into the joint space created by the surgery (D). Below: Display of the Medtronic StealthStation S7 workstation. All images courtesy of Miyazaki et al. Licensed under CC BY 4.0.
Above: Intraoperative photos demonstrating a bony fusion between the condylar head and glenoid fossa (A), the use of the navigation system to confirm the operating position (B), the formed articular cavity (C), and the temporal muscle insertion into the joint space created by the surgery (D). Below: Display of the Medtronic StealthStation S7 workstation. All images courtesy of Miyazaki et al. Licensed under CC BY 4.0.Because the patient's skull was measured at 0.7 mm at the thinnest point and the navigation system error was determined to be 0.3 mm, the clinicians decided to perform a 10-mm-wide osteotomy and TMJ release. As a final step, the temporal muscle and fascia were inserted into the glenoid fossa created by the surgery as interpositional materials.
Results of surgery
The day after surgery, the patient started mouth-opening training. Six months following surgery, the girl's maximum oral aperture was 38 mm (compared to 13 mm before the operation) and her mouth motility was restored. No complications after surgery were reported.
A follow-up CT showed a loss of bony adhesions in the condyle and glenoid, improvement of the condylar deformity, and the joint cavity intervention, the authors wrote.
Even though the surgery in this case was a success, Miyazaki et al reported some drawbacks with this particular electromagnetic navigation system, including the system's error value and its required setup time after the general anesthesia had been started.
According to the authors, navigation systems have been reported to improve quality and reduce risk in skull base surgeries, since they help the surgeon keep the skull base stable and enable higher cutting precision and greater control over the amount of bone removed.
This case is one of only a few where similar navigation systems were used to surgically treat pediatric patients diagnosed with TMJ ankylosis. Though early surgery for TMJ ankylosis is recommended, the appropriate surgical technique and materials to use are still a matter of debate. Cases involving pediatric patients also have an added element of danger, as children have smaller skull widths than adults, which can lead to surgical complications such as brain damage.
"A surgical navigation system makes it possible to achieve real-time positioning during surgery and to transfer the preoperative design to the actual operation," the authors wrote.