If you count on your computer-aided detection (CAD) application to help you find breast lesions, you might want to pay attention to which mammography projections your CAD actually marked. And then look at them both again.
A study from the Elizabeth Wende Breast Clinic in Rochester, NY, found that CAD was a bit more sensitive for cancer detection in craniocaudal (CC) images than in mediolateral oblique (MLO) views, although CC views also produced more false-positives. And, like human readers, CAD tended to see different kinds of lesions more frequently depending on the projection.
Some breast cancers aren't found at the initial examination, and may manifest as interval cancers, said Dr. Stamatia Destounis, a radiologist at the center and clinical associate professor at the University of Rochester in Rochester, NY.
Lesions can be missed for many reasons, of course. Sometimes a lesion isn't recognizable as such on both projections, or its appearance differs on MLO and CC projections, or it is located in the posterior chest, or surrounded by dense breast tissue.
Some missed lesions are actually detected by CAD on one view or the other and dismissed, or seen retrospectively. Some visible lesions have been ignored when radiologists "didn't believe it was a cancer unless they could see it on both views," Destounis said in a presentation at the 2007 Computer Assisted Radiology and Surgery (CARS) meeting in Berlin.
CAD has been shown to aid overall cancer detection, and has become an important component of breast imaging protocol at Elizabeth Wende, where its use has been the standard of care since 2000, Destounis said.
In a 2001 retrospective review, Freer and colleagues found that 71% of breast cancers had been marked by CAD a year before they were diagnosed, Destounis said (Radiology, September 2001, Vol. 220:3, pp. 781-786).
In a later Radiology paper, Destounis' group concluded that breast CAD could potentially decrease the false-negative rate at double reading by more than a third, from 21% to 19%. (Radiology, August 2004, Vol. 232:2, pp. 578-584).
But it was a 1978 study by Andersson and colleagues (and later studies by Kopans et al, and Brown et al) citing different lesion appearance on different mammo views that inspired the present study about how different mammography projections might impact CAD results, Destounis said (Andersson et al, American Journal of Roentgenology, February, 1978, Vol. 130, pp. 349-351).
The previously demonstrated variability mirrored their own experience, according to Destounis. "We were able to use CAD to detect cancer, and we found that CAD has sensitivities of 93%-100% for calcium," she said. "However, for masses it was 60%-80% depending on what kind of mass it was, whether it was lobular or ductal cancer, etc. And we felt it was also important to determine whether the CAD marked the cancer differently on the craniocaudal (CC) or mediolateral oblique (MLO) view, and to evaluate the effect of lesion type, mass, calcium, architectural distortions, or asymmetry on CAD's ability to mark the lesion."
Her group reviewed 45 biopsy-proven cancers in 44 breast cancer patients, all of which had been initially detected on digital mammography (Senographe, GE Healthcare, Chalfont St. Giles, U.K.) and with CAD (ImageChecker Version 8.3.15, R2 Technology, Sunnyvale, CA).
After detection at mammography with CAD, 279 suspicious lesions were referred to needle core biopsy, where cancer was revealed in the 45 lesions reviewed in the retrospective study.
"In order to be included they had to be biopsy-proven cancers, and the lesions had to be seen both on MLO and on craniocaudal views," Destounis said.
The patient data listed age, BI-RADS density (fatty, scattered, heterogenously dense, or extremely dense) lesion type (asymmetric density, mass, calcification, mass with associated calcification, architectural distortion) and the BI-RADS assessment category, and whether the lesion was seen on MLO, CC, views or both, she said.
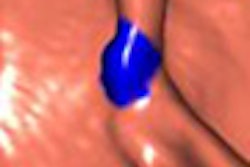
 |
| CAD reveals true-positive cancer with two marks on MLO view, 1 mark on CC view. All images and data courtesy of Dr. Stamatia Destounis. |
The median patient age was 53 years (range 29-84), and cancers were found in 27 screening and 17 diagnostic patients.
"Concerning densities, 59% (of the cancers) were in heterogenously dense breast tissue," and 13 in patients with dense breasts, Destounis said. CAD sensitivity fell with increasing breast density. The densities presented as four asymmetric densities, 16 masses, 19 calcifications, four masses with calcifications, and two architectural distortions.
"The median lesion size was 1.8 cm, however, there was a range of half cm to 5.9 cm, and a median of four CAD marks per case, and a range of 0-13 marks," Destounis said. "Fifty-eight percent (n=26) of the cases were invasive cancers, 40% (n=18) were ductal in-situ carcinomas (n=18), and one was an atypical ductal hyperplasia (2%) that was recommended to open surgical biopsy."
At surgery, 10 cases were upgraded from in situ to invasive disease, for a total of 40/45 invasive cancers, she said. Eight of the 10 upgraded cancers were detected by CAD, she noted, including eight seen in both MLO and CC views, one found in the CC view only, and one tumor not seen on either projection or CAD.
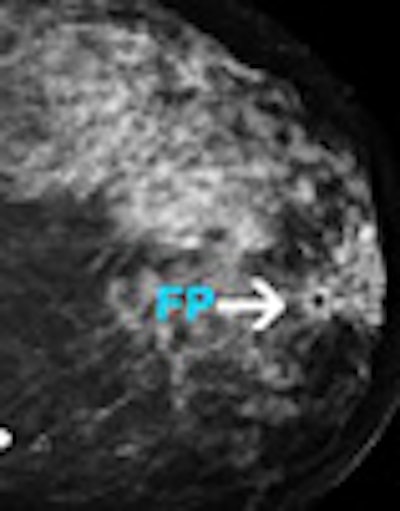
 |
| Left MLO view and the left CC view of a 52-year-old screening patient. CAD didn't mark the cancer on either view; density can be seen in the left superiolateral aspect. Biopsy revealed invasive carcinoma. |
"Thirteen of the 16 masses were detected by CAD for 81% detection," Destounis said. "One hundred percent of the calcifications and 100% of the masses (n=4) with calcium were detected by CAD, and 100% of the architectural distortions, so 39 (of 45) cases were marked by CAD."
What did CAD find where? Three of the masses were detected on MLO, six at CC, and four on both projections. Among the calcifications, 60 were detected on both MLO and CC, two on CC alone, and one on MLO alone.
CAD's overall case sensitivity, i.e., the number of lesions CAD marked compared to the number of lesions visible on both views, was 87%, or 39/45 cases. CAD found four of the lesions on MLO only, eight on CC only, and 27 in both views. Thus, image sensitivity was 78% on CC views, compared to only 69% on MLO views, Destounis said.
Breaking the results down by lesion type, CAD found 19 of 19 calcifications (100%), one of four asymmetries (25%), 13/16 (81%) masses, four of four masses with calcifications (100%), and two of two architectural distortions (100%).
CAD detected the asymmetric densities in both MLO and CC views. For the masses, three were detected on MLO, six at CC, and four on both views. Among the calcifications, 60 were detected on both MLO and CC, two on CC alone, and one on MLO alone. CAD detected all masses with calcification and architectural distortion on both views.
 |
| CAD was most sensitive for calcifications, masses with calcifications, and architectural distortions (100% for all), followed by masses (81%). |
Overall case sensitivity, i.e., correctly marked lesions on either view, was 39/45 or 87%. But CAD did better on CC views.
"When you take the lesions marked for every view over the number of cases we know are visible on both CC and MLO views, the image sensitivity was 69% (31/45) for MLO and 78% (35/45) for the CC view," she said.
Just over half (54%, 106/198) of the total CAD marks were false positives, Destounis reported. Most (81/108) were calcium marks, while 25/108 were masses. Of the false positives, 37% were in the MLO view, compared to 63% in the CC view.
"At our clinic, the CAD sensitivity setting is set for balanced sensitivity in masses and increased sensitivity in calcifications," she said. "Therefore, we can postulate that a proportion of the false-positive CAD marks gotten in our study are a function of these settings chosen over time."
 |
| Sensitivity results show variable CAD sensitivity based on lesion type and mammography projection. CAD found the greatest number of masses on craniocaudal views. |
 |
CAD has demonstrated the capability to detect visible cancer in standard mammography projections, Destounis concluded.
"In this particular study cohort, the craniocaudal view was found to provide CAD with the most definitive features for lesion recognition," she said. "Further evaluation of the false-positive marks and the specific features of the lesions not marked by CAD is needed."
By Eric BarnesAuntMinnie.com staff writer
August 6, 2007
Related Reading
CAD still not out of the woods, despite Oregon payor's reversal, July 24, 2007
Oregon payor reverses stand, reinstates CAD payments, July 23, 2007
NEJM study prompts Oregon payor to cancel CAD reimbursement, July 11, 2007
Studies show CAD matches up well with CR mammo, FFDM, May 24, 2007
NEJM study pans CAD, draws attention and criticism, April 5, 2007
Copyright © 2007 AuntMinnie.com