Computer-aided detection (CAD) technology in radiology has largely focused on cancer applications in the breast, chest, and colon. But with the pace of innovation slowing in those fields, the development of new musculoskeletal CAD applications could help revitalize the technology.
In musculoskeletal radiology, CAD may offer significant value in assisting radiologists with tedious clinical tasks such as labeling pathology and detecting, characterizing, and visualizing bone fractures, according to Dr. Ty Bae, Ph.D., chair of radiology at the University of Pittsburgh Medical Center. CAD could also shine in quantification tasks such as bone age assessment, arthritis grading, and cartilage assessment.
Close collaboration between clinicians and researchers will facilitate these types of clinically targeted applications, Bae said.
"[Then] we can make useful CAD, make it usable, and to use it," Bae said. He shared his thoughts on the promise of musculoskeletal CAD during a talk at the 2009 RSNA meeting in Chicago.
CAD research and development has been largely focused to date on task-specific clinical applications and has been stimulated by cancer screening initiatives that target the breast, chest, and colon. Other niche areas for CAD include interstitial disease, pneumothorax, pulmonary embolism, vessel tracking/stenosis, liver or brain tumors, and musculoskeletal applications.
However, a perception has emerged among some that CAD is in decline, Bae said. Although current algorithms feature fast computation power, no major algorithmic breakthroughs have been achieved, he said.
With the technology's questionable clinical impact and the lack of imaging-based cancer screening, there's a sense that grants from the U.S. National Institutes of Health (NIH) are drying out and researchers are leaving CAD, Bae said.
"And from the industry point of view, there is a limited return on investment," he said.
Also complicating things has been an impasse at the U.S. Food and Drug Administration (FDA), which has largely frozen CAD regulatory submissions while it sorts out an initiative to change the way it regulates the technology.
Revitalizing CAD
For CAD to be revitalized, clinically relevant and targeted applications must be developed, Bae said.
"This requires close clinician involvement in CAD development and you've got to bring value to patient care," Bae said.
CAD must also be integrated with PACS, eliminating the need for radiologists to move to a different workstation. In addition, the superiority of CAD over traditional methods should be 100% clear, Bae said.
"[CAD] has got to be better than standard clinical interpretation and provide [a] more efficient and cost-effective tool," he said. "This can improve reimbursement and clinical acceptance."
In developing CAD, it's important to understand the technology's strengths and weaknesses. For example, CAD performs at its best in handling tedious tasks (such as detecting small lung nodules and counting ribs) and jobs requiring pixel-by-pixel navigation (such as boundary detection and quantification), Bae said.
CAD is not commonly available or used in musculoskeletal imaging applications today. Musculoskeletal cancers are rare, and no screening is performed, unlike the current CAD domains in the breast, chest, and colon, Bae said.
Bone fracture is a common musculoskeletal clinical application, but there is no practically usable CAD system for this, Bae said. Bone fractures can be difficult to detect due to the need to consider multiple bones, complex bone morphology, and variable bone density. With that in mind, CAD would add the most value in reducing the workload of the radiologist, he said.
For example, CAD can count ribs and vertebrae, taking over a tedious task for the radiologist. The labeling of fracture fragments in the complex hand and ankle bones would also be useful for treatment, he said.
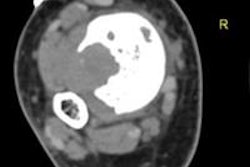
 |
| Axial CT images show three fractures involving the sixth, seventh, and ninth ribs (arrows), while the bony thorax and rib fractures are also displayed in 3D volume-rendered images. The use of CAD to automatically label and index fractured ribs could save time during the interpretation and reporting process. All images courtesy of Dr. Ty Bae, Ph.D. |
A number of published studies have found CAD to be promising in counting ribs and vertebrae on CT. All have used only normal bony structures, however, Bae said.
That might be a problem, as CAD may not be effective in bone deformity cases such as scoliosis or osteoporosis or in areas with limited anatomic coverage. "So CAD is not available for clinical cases where CAD is really needed," he said.
Researchers have also found promising results using CAD technology to provide semiautomated reconstruction of highly fragmented bone fractures. In addition, CAD algorithms have also been evaluated for detecting bone lytic metastases, metastasis in the ribs, and periprosthetic osteolysis, as well as abnormalities and changes on bone scans.
Quantitative imaging
CAD offers potential in musculoskeletal quantitative imaging applications such as assessing bone, evaluating bone quality via bone trabecular structure analysis, and quantifying and characterizing osteoarthritis and rheumatoid arthritis, Bae said.
Bone age assessment via a left-hand radiograph is a common pediatric radiologic exam, but it's time-consuming and can be variable depending on the reader, Bae said. CAD technology, however, may be able to perform this task in automated fashion. A recent study found that the use of CAD to assess bone age yielded a mean difference of 0.5 years compared with readings by two radiologists.
The trabecular structure of bone can provide clues to fracture risk, and researchers have demonstrated the use of CAD to perform various texture analyses on radiographs and also to evaluate bone quality using topology parameters on high-resolution MRI images, Bae said.
The characterization and quantification of arthritis is also a promising area for CAD. For example, researchers have explored the use of CAD to provide semiautomated measurements of interphalangeal joint space in the fingers, to automatically detect bone erosions in rheumatoid arthritis patients, and to assess disease progression in knee osteoarthritis, Bae said.
CAD tools can also be quite useful in segmenting knee cartilage on MRI scans. In recent research performed at the University of Pittsburgh, a semiautomated method was 10 times faster and more reproducible than manual segmentation, Bae said.
 |
| Semiautomated segmentation of knee cartilage (left) was found to closely agree with a manual delineation method (right), and was also more efficient and reliable. |
By Erik L. Ridley
AuntMinnie.com staff writer
February 12, 2010
Related Reading
Software saves time by segmenting meniscus in knee MR images, February 1, 2010
Integrating CAD with PACS adds clinical value, December 18, 2009
CAD may improve novice performance in pulmonary CTA, March 26, 2009
NY Times story focuses on CAD approval, January 15, 2009
CAD shows potential for knee MR studies, May 26, 2008
Copyright © 2010 AuntMinnie.com