Duke University researchers have developed a 10-point scale that can simplify the assessment of multiple abdominal x-ray reports of infants with clinical symptoms of necrotizing enterocolitis, helping to predict the severity of the disease.
Use of the 10-point Duke abdominal assessment scale (DAAS) can help clinicians better evaluate the condition of their patients, as well as expedite the accurate identification of infants in need of intense medical surveillance and potential surgical intervention.
Published in the November issue of the American Journal of Roentgenology, the study (2009, Vol. 193, pp.1408-1413) compliments previous research conducted to measure and validate the consistency of reporting using the standard lexicon of the DAAS scale by pediatric radiologists (2008, Vol. 191, pp. 190-197).
Necrotizing enterocolitis is a severe intestinal inflammatory disease of the intestinal tract that is associated with significant morbidity and mortality. Neonates and infants who exhibit clinical suspicions typically have abdominal x-rays performed every six to 12 hours while they receive antibiotics intravenously and have bowel rest.
Although ultrasound is starting to be used, abdominal x-ray remains the primary imaging procedure to assess disease progression and to help determine if surgical intervention is needed. Because no single physical, laboratory, or radiographic finding is typically specific enough to make a diagnosis of necrotizing enterocolitis, the diagnosis tends to be based on a composite of clinical and radiographic findings.
|
Duke abdominal assessment scale (DAAS) scoring system
|
In 2005, to improve report consistency and reduce the variability of terminology contained in multiple radiology reports, radiologists at Duke University Medical Center in Durham, NC, developed a 10-point scale of abnormal findings associated with necrotizing enterocolitis. By assigning a numeric score that increases with the severity of symptoms, the objective is to create a clear, concise radiology report using standard terminology that provides clinicians with consistency of identified findings. This, in turn, makes comparing and analyzing multiple reports easier for the clinicians receiving them.
When the DAAS scale had been routinely used for 18 months, researchers conducted a formal study to measure the level of consistency of using DAAS to corroborate abnormal x-ray findings identified by a number of readers. Four pediatric radiologists representing the spectrum of career experience interpreted 88 abdominal radiographs. The results of the study revealed substantial intraobserver and interobserver agreement.
However, the researchers did not evaluate clinical outcomes of the patients to determine if progression on the 10-point scale correlated with the severity of disease. This was the objective of the second study, according to Dr. Caroline Hollingsworth, assistant professor of radiology at Duke University School of Medicine and the principal investigator for both studies.
The study group consisted of 43 patients with symptoms of necrotizing enterocolitis who underwent surgical exploration for suspected abnormalities of the small bowel or colon between July 1, 2000, and November 30, 2007. For all patients, the initial and follow-up radiographic series were evaluated, but only the initial radiographic series was used in the data analysis because 20 of the 43 patients were shown to have developed pneumoperitoneum on the second film in the series.
The control group consisted of all neonatal ICU patients younger than 2 months who had at least one two-view abdominal radiographic series obtained between July 1, 2005, and June 30, 2006. Of the 297 patients with an indication for abdominal radiography consistent with suspected necrotizing enterocolitis, 86 were randomly selected. For each patient in the control group, one two-view radiographic series was randomly selected.
The average patient age was 26.7 days at the time the radiology exam being used in the study was taken, and for the control group, the average age was 22.6 days. In the study group, 39.5% of the patients were girls, compared with 51.2% in the control group.
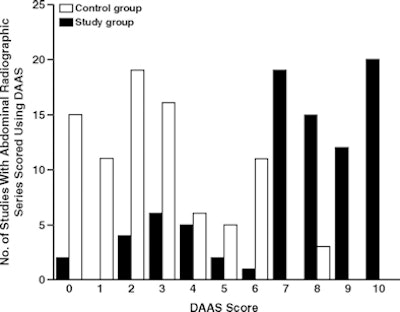
Each two-view radiographic series was scored by consensus by two pediatric radiologists who had used the DAAS scale in reporting for two years. Their assessment is summarized in the following graph:
 |
| Distribution of DAAS scores in control group patients (n = 43 patients; 86 initial and follow-up studies) and study group patients (n = 86 patients). Note that control group radiographic series had overall lower scores than study group radiographs. Mean DAAS score for control group was 2.7 and for study group, 7.3. Graph courtesy of the American Journal of Roentgenology. |
The DAAS scale accurately differentiated severe disease from potentially milder disease, according to these results. For every one-point increase in the DAAS scale, patients were statistically significantly more likely to have severe necrotizing enterocolitis, as indicated by eventual surgical intervention.
"The DAAS scale is a good communications tool about whether the patient is trending better or worse," Hollingsworth told AuntMinnie.com. "Because it shows a simple consistent pattern of findings, our clinicians and surgeons use it as a kind of barometer, and if our residents dictate a report without a DAAS rating, the clinicians call to request it."
By Cynthia E. Keen
AuntMinnie.com staff writer
December 30, 2009
Related Reading
Color Doppler ultrasound a sensitive way to diagnose bowel necrosis in neonates, May 2, 2005
Copyright © 2009 AuntMinnie.com