The U.S. medical imaging community is experiencing both anticipation and angst as Congress and the Obama administration prepare to tackle rising healthcare spending. Many imaging observers are concerned that the government may repeat recent history by approaching imaging reimbursement with a hatchet rather than a scalpel.
Former Secretary of Health and Human Services Mike Leavitt said in December that Medicare is "drifting toward disaster," and that Congress and the new administration should implement Medicare reform this year to improve the U.S healthcare system. Many Capitol watchers also believe that the Obama administration may want to cut costs in some areas of Medicare and Medicaid to free up funds in other areas, such as expanding access to care.
Imaging services are an easy target. Imaging is one of the fastest growing areas of healthcare spending, with federal payments for imaging rising from $7 billion in 2000 to $14 billion in 2006. That's an average annual growth rate of 13%, according to the Congressional Budget Office (CBO). Spending for advanced imaging procedures, such as MRI and CT, grew even faster at a 17% annual rate.
Imaging industry proponents are watching the maneuvering with some trepidation. In particular, many Capitol watchers are nervous about a repeat of the Deficit Reduction Act (DRA) of 2005, when Congress slashed Medicare reimbursement for outpatient imaging services as part of an 11th-hour move that was implemented with little data or input from the imaging community.
The CBO report
The urgency of the task was underscored by a CBO report in December 2008 that suggested a number of changes in Medicare payment policies for medical imaging services. The report lists 115 options for reducing (or in a few cases, increasing) federal spending on healthcare.
Options that pertain specifically to medical imaging include:
- Modifying the equipment utilization factor
- Requiring prior authorization for advanced imaging services
The equipment utilization factor is basically the Centers for Medicare and Medicaid Services' (CMS) estimate of the percentage of time that equipment is in operation at a healthcare practice. Currently, that utilization factor is 50%, but if the factor is raised, it would spread the cost of the equipment over more units of service, resulting in a smaller payment per service, according to the report.
For example, if the equipment utilization factor were raised from 50% to 75%, Medicare would save $130 million in 2010 and $970 million from 2010 to 2014. If the factor were raised to 95%, Medicare would save $200 million in 2010 and $1.45 billion from 2010 to 2014.
In supporting the option, the CBO report noted that data presented by the Medicare Payment Advisory Commission (MedPAC) in a June 2006 report to Congress indicate that the average rate of MRI scanner use was 91% and the average rate of CT scanner use was 73%. MedPAC is expected to recommend the factor be moved from 50% to 90% in its March 2009 report to Congress.
 |
| Dr. James Thrall, chairman of the ACR Board of Chancellors. |
The impact of such a change could be so great that it affects access to imaging services, as noted in the CBO report. Rural practitioners might be discouraged from providing imaging because they might not use the equipment often enough to cover the capital costs incurred in purchasing it, the report notes.
Requiring preauthorization
Option 41 in the CBO report is to require preauthorization for imaging services. Although anathema to imaging providers, the concept is beginning to win increased attention from government regulators who are looking for a way to reduce imaging utilization that's more proactive than driving down reimbursement after the scan has already taken place.
The CBO report notes that private payors are already using preauthorization, and Medicare could begin to do so by hiring radiology benefits management firms to make decisions on its behalf as to whether to approve payment for a specific imaging service. The report notes that Medicare could save $20 million starting in 2011 and $220 million from 2010 to 2014 by implementing preauthorization.
The self-referral question
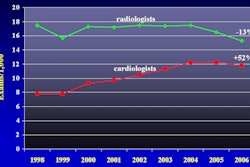
As policymakers prepare to attack rising imaging costs, radiology's proponents try to make their point that much of the growth in imaging utilization is coming from in-office physician self-referral as nonradiologist physicians adopt imaging technology.
CMS has made halting efforts to tackle self-referral, with one mechanism being the so-called antimarkup rule, established in 2007 but not put into effect until 2009. The rule states that, except under certain circumstances, physicians can't profit from a test ordered when their practice bills for that test.
However, exceptions to the rule have become so commonplace that many physician practices will find a way to escape its impact, at least with respect to the technical component of imaging services. The CMS has proposed revisions to the rule, and some feel the exceptions have practically swallowed the rule's intent.
 |
| Thomas Greeson of law firm Reed Smith. |
Another proposal that could clamp down on physician self-referral is a requirement that physician groups that want to bill Medicare for imaging enroll as independent diagnostic testing facilities (IDTFs) and be subject to the standards that govern them. This includes rules on staff licensure, proficiency requirements for supervising physicians, and prohibitions on sharing, leasing, or subleasing equipment.
Some imaging observers believe that many nonradiology practices may simply stop offering imaging altogether rather than go through the hassle of qualifying as an IDTF.
Another recent government initiative that could slow down physician self-referral is accreditation. The Medicare Improvements for Patients and Providers Act (MIPPA) of 2008 mandated that all nonhospital providers of imaging services must be accredited and meet quality requirements by 2012.
CMS will be required to select accrediting bodies by 2010, and both the ACR and the American College of Cardiology are involved in formulating an approach to accreditation for CMS.
"The [ACR] has an outstanding program in place, and we would like to be deemed by CMS as a provider of those accreditation services," Thrall said.
MIPPA revisited?
Legislators may also revisit the sustainable growth rate (SGR) formula for setting the Medicare Physician Fee Schedule (MPFS), which mandates cuts in physician payments whenever real growth in healthcare spending outstrips projected growth. Many healthcare observers believe the calculations underlying the SGR are fatally flawed; for example, the SGR would have required a 10.6% pay cut in the MPFS last year unless Congress took action.
The passage of MIPPA temporarily averted that pay cut, but the SGR formula is still in place, and another MPFS reduction is looming unless Congress takes action.
"There's now a strong appetite in Congress for a longer-term and ideally permanent solution to this flawed SGR formula," Thrall said. "It really just takes a huge amount of time, energy, and effort for Congress to go through this each year to no real lasting change or benefit."
Don't be hasty
As recommendations like the CBO report continue to flow in Washington, policymakers feel the pressure to find a timely solution to a flawed healthcare system. But rushed policies could mean trouble.
Greeson said Congress would be unwise to jump immediately on the CBO recommendations.
"They need to let some of Medicare's initiatives percolate, like the antimarkup rule and the IDTF performance standards," Greeson said.
And, he added, the possibility of a Democratic Congress and the Obama administration looking toward imaging as a funding vehicle to reduce spending and direct the savings to other areas would be a serious mistake. "Further cuts could have a significant impact on access.... Congress should not adopt across-the-board cuts ... and should tailor their policy response to the root cause of the increased utilization," Greeson said.
A voice for imaging
With the uncertainty of the coming legislation in 2009, some organizations such as the Medical Imaging and Technology Alliance (MITA) in Roslyn, VA, will continue to work with what is in place.
 |
| Ilyse Schuman, managing director of the Medical Imaging and Technology Alliance. |
For medical imaging, the implementation of broad and sweeping changes as exemplified by the DRA is a major concern.
"One size does not fit all," Schuman said. "What works in large urban areas is very different from what's happening in rural areas. Or it's different depending upon the age and health condition of a patient and, unfortunately, both the CBO and MedPAC options ... were based on a survey that was really not representative of what's going on across the nation."
It remains to be seen whether the Obama administration will be more or less sympathetic to efforts to rein in spending in radiology.
"I think the new Congress and administration are going to be very distracted by what's happening with the economy," Thrall said. "One of the issues that has already come up is how healthcare will play a role in turning the economy around. What opportunities are there in healthcare to pump money into the economy in a way that will have a stimulatory but also lasting benefit to the health system? One obvious point is to include healthcare IT as part of the stimulus package."
By Lin Muschlitz
AuntMinnie.com staff writer
January 27, 2009
Related Reading
2009 MPFS proposal: If you're not an IDTF, you'll be one soon, July 10, 2008
Beware, AMIC says: The DRA could be the least of it, June 10, 2008
ACR update: Teaching Congress how to fish, May 7, 2008
Copyright © 2009 AuntMinnie.com