Bronchiolitis Obliterans Organizing Pneumonia (BOOP):
Cryptogenic Organizing Pneumonia (COP)
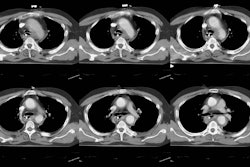
View Images of BOOP/COP
Clinical:
Bronchiolitis obliterans with organizing pneumonia (BOOP) is a histologic description and not a specific diagnosis. Etiologies of BOOP include toxic fume or dust inhalation (extrinsic allergic alveolitis), post infectious (mycoplasma, fungal, or viral), connective tissue disease (idiopathic inflammatory myopathies, rheumatoid arthritis, Sjogren's syndrome [9]), smoking, chronic graft-vs-host disease, organ transplantation, and drug toxicity. Bleomycin, gold salts, cyclophosphamide, and methotrexate are the most common drugs associated with this form of lung injury [8]. Amiodarone, nitrofurantoin, penicillamine, and sulfasalazine are less common causes of drug induced BOOP [8]. BOOP has also been described in the contralateral lung following radiation therapy [6]. Commonly an etiologic factor is not identified and the condition is idiopathic (cryptogenic) in up to 50% of cases.
Idiopathic BOOP is also referred to as "cryptogenic organizing pneumonia". Most cases of idiopathic BOOP occur in patients between the ages of 40 and 60 years and there is no sex predilection. Patients generally present with a history of a flu-like illness prodrome with a dry, non-productive cough that lasts 2 to 12 weeks, malaise, gradual dyspnea, and a low-grade fever. There is no association with smoking [9]. The ESR is elevated and greater than 60 mm in about 30% of patients [9]. Pulmonary function studies usually demonstrate restrictive abnormalities. On bronchoalveolar lavage the differential white count may show a characteristic "mixed pattern" with increased lymphocytes (20-40%), neutrophils (about 10%), and eosinophils about 5%) [9]. The lymphocyte CD4/CD8 ratio is decreased [9].The diagnosis should not be made without biopsy confirmation [7]. There is NO response to antibiotics, but the process often has a good response to treatment with steroids. Clinical manifestations improve within 48 hours of initiation of therapy, but complete resolution of radiographic infiltrates usually takes several weeks. The duration of treatment is variable, but is usually between 6 and 12 months [9]. Relapses may occur following cessation of steroid therapy in about one-third of cases [2], and do not indicate a potential negative outcome [9]. Overall prognosis for typical BOOP (patchy alveolar opacities) is excellent following steroid therapy [9]. Factors associated with a poor outcome include a predominantly interstitial pattern on imaging, lack of a lymphocytosis on BAL fluid, and an associated underlying disorder [9].
BOOP is referred to as a proliferative bronchiolitis- on histologic analysis, there is obliterative granulation tissue plugs (Masson bodies) found within the lumen of the small airways (alveolar ducts and respiratory bronchioles) due to bronchiolar epithelial damage (bronchiolitis obliterans). Organizing pneumonia is seen in the surrounding lung parenchyma. A constrictive bronchiolitis with concentrically scarred/ stenotic bronchioles may also be noted histologically, but this is not the characteristic finding associated with BOOP.
X-ray:
CXR: The radiologic manifestations of BOOP are those of an organizing pneumonia. On CXR there is bilateral patchy, peripheral alveolar infiltrates (organizing pneumonia) or ground glass opacities in over two-thirds of cases. The consolidations are predominantly subpleural in up to 50-60% of patients. Unilateral, focal, or lobar consolidations are seen less commonly. All lung zones may be affected. Diffuse small linear and nodular opacities are seen in 20-40% of cases. A reticular interstitial pattern is found in a minority of cases. The disorder can progress to fibrosis, but honeycombing is usually absent. Effusions are noted in 10% of cases on plain film and adenopathy is not usually identified.
Computed tomography: On HRCT, subpleural, patchy, basilar dense consolidations (80-90%) with air bronchograms and/or ground-glass densities (60%) producing a pattern of mosaic attenuation are the characteristic findings (in up to 50% of affected patients, especially the immune compromised), but this finding is non-specific as it may also be seen in chronic infection (TB, MAI), sarcoidosis, alveolar cell carcinoma, lymphoma, and chronic aspiration. Large, peripheral areas of irregularly marginated mass-like consolidation have also been described and may be seen in up to 20% of cases [5].
Peribronchial thickening is common. Centrilobular nodular densities ranging in size from 1 to 10 mm (sometimes larger), which may be well or poorly defined, may also be seen (30-50% of cases) and correlate with areas of organizing pneumonia. Adenopathy is more commonly noted by CT (25%) and effusion is found in up to 30% of cases [3]. The presence of dense consolidations helps to distinguish BOOP from DIP, and fibrosis is also not observed in BOOP.
REFERENCES:
(1) RadioGraphics 1996;16:1009-1033
(2) AJR 1997; Collins J, et al. Ground-glass opacity at CT: The ABCs. 169: 355-367
(3) J Thorac Imaging 1995;10 (4):236-254 (p.249-250)
(4) ARRS 1996, View box exhibits #459-60
(5) AJR 1998; Akira M, et al. Bronchiolitis obliterans organizing pneumonia manifesting as multiple large nodules of masses. 170: 291-295
(6) Respir Medicine 1997; van Laar JM, et al. Bronchiolitis obliterans organizing pneumonia after adjuvant radiotherapy for breast carcinoma. 91: 241-244 (No abstract available)
(7) AJR 1994; Garg K, et al. Proliferative and constrictive bronchiolitis: Classification and radiologic features. 162: 803-808
(8) Society of Thoracic Radiology Annual Meeting 2000 Course Syllabus; Erasmus JJ. Pulmonary drug toxicity: Pathogenesis and radiologic manifestations. 65-68
(9) Thorax 2000; Cordier JF. Organizing pneumonia. 318-328 (Review- No abstract available)