CHICAGO – With its ability to decipher plaque composition, multidetector-row CT is as good as intracoronary ultrasound for detecting rupture-prone soft coronary lesions, according to German researchers.
Dr. Andreas Kopp from the Karl Eberhardt University in Tübingen presented the results of his group’s study at the RSNA on Sunday. They compared multidetector-row CT (MDCT) to intracoronary ultrasound (ICUS), the gold standard for the non-invasive imaging of coronary artery disease.
“The noninvasive detection of coronary artery disease is a prime goal for future development in clinical imaging,” Kopp said, pointing out advantages of MDCT such as simultaneous acquisition of multislice images, the ability to cover a large volume in a given time, and high temporal resolution.
The study sample consisted of 20 patients who were scheduled for ICUS-guided percutaneous transluminal coronary angioplasty. A four-slice CT system with a 500 millisecond rotation time and a retrospectively electrocardiographically gated (ECG) spiral scan technique was used (Somatom VolumeZoom, Siemens Medical Systems, Erlangen, Germany).
The protocol for the coronary CT angiography allowed for covering the heart within a 25-second breath-hold, 4 x 1 mm collimation, and ECG-gated image reconstruction. Each patient was given 120-150 ml of nonionic contrast agent at a flow rate of 4 ml per second.
ICUS was performed under fluoroscopic guidance. Continuous ultrasound images were obtained with an UltraCross 3.2F, 30 MHz coronary imaging catheter, Kopp said.
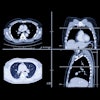
One section of plaque was selected in each patient and defined as soft, intermediate, or calcified. According to the results, MDCT identified 10 soft plaques, two intermediate, and eight calcified plaques. ICUS pinpointed the same number, Kopp said.
However, on ICUS, soft plaques appeared as hypoechogenic areas, suggesting the presence of lipid cores. Soft plaque was defined as 80% of the plaque area with an echogenicity lower than the adventitia, Kopp said.
“With MDCT, these plaques were clearly detectable and could be classified as soft plaques,” Kopp said. In total, MDCT was able to identify 37 out of 40 plaques. Three areas of plaque were seen retrospectively as small, soft, flat plaques after the radiologists were unblinded to the ultrasound results, he added.
The advantage of using MDCT could lie in its ability to detect plaque early and prevent rupture, particularly when paired with information documenting high grade stenoses. It may also serve as a tool for risk stratification, he said.
An audience member asked how the investigators pinpointed calcified plaque give the degree of opacificaton on the post-contrast CT images. Kopp said that pre-contrast scans were essential to prevent confusion between calcification and opaque areas.
By Shalmali Pal
AuntMinnie.com staff writer
November 27, 2000
Related Reading
Copyright © 2000 AuntMinnie.com
Click here to view the rest of AuntMinnie’s coverage of the 2000 RSNA conference.
Click here to post your comments about this story.