The traditional treatment of uterine fibroids in patients who wish to become pregnant is surgical removal by myomectomy. However, the minimally invasive interventional procedure of uterine fibroid embolization has a lower complication rate and has a comparable fertility rate to myomectomy after treatment, according to researchers from the United Arab Emirates.
Uterine fibroids
Uterine fibroids are benign tumors in the uterus that can cause prolonged, heavy menstrual bleeding that can be severe enough to cause anemia or require transfusion. Patients may also have disabling pelvic pain and pressure, urinary frequency, pain during intercourse, miscarriage, interference with fertility, and an abnormally large uterus resembling pregnancy.
 Dr. Jamal Alkoteesh is the chief of interventional radiology and chairman of radiology at Al Ain Hospital in the United Arab Emirates.
Dr. Jamal Alkoteesh is the chief of interventional radiology and chairman of radiology at Al Ain Hospital in the United Arab Emirates.Approximately 15% to 30% of Arabic women who are 35 and older have uterine fibroids. An increasing number of women are delaying pregnancy until their late 30s, which is also the most likely time for fibroids to develop.
The impact of uterine fibroids on pregnancy, the risk, and type of complications appear to be related to their size, number, and location. Certainly, infertility results when fibroids grow large enough that they obstruct one or both of the fallopian tubes. Additionally, fibroids are associated with a higher rate of miscarriage when they grow into the cavity of the uterus where embryos implant (i.e., submucus or intracavitary).
The traditional treatment of uterine fibroids in patients who wish to become pregnant is surgical removal by myomectomy. This treatment is usually effective, particularly if the fibroid is single and subserosal in location, the fibroids are in small number, and they are small or medium in size.
The minimally invasive interventional radiology procedure of uterine fibroid embolization (UFE) has a lower complication rate than myomectomy. It may be performed if a woman has a single fibroid, many fibroids, or large-sized fibroids and a gynecologist cannot rule out a hysterectomy during myomectomy, myomectomy is unsuccessful, or when fibroids recur after myomectomy. The procedure may also be performed for women who want to avoid surgical removal for culture reasons, surgically high-risk women with fibroids, women of any age with fibroids who want to preserve their uterus and avoid the psychological trauma of hysterectomy, and, more important, in unmarried virgin women with fibroids.
 A 34-year-old woman presented with menorrhagia for nine days. The patient also had rheumatic mitral valve stenosis. Ultrasound scan of the uterus before embolization showed a 10 x 8-cm uterine fibroid with tense vascularity, which was treated by UFE. All images courtesy of Dr. Jamal Alkoteesh.
A 34-year-old woman presented with menorrhagia for nine days. The patient also had rheumatic mitral valve stenosis. Ultrasound scan of the uterus before embolization showed a 10 x 8-cm uterine fibroid with tense vascularity, which was treated by UFE. All images courtesy of Dr. Jamal Alkoteesh.Key findings & Arab Health 2016
Uterine fibroid embolization blocks blood supply to treat painful uterine fibroids, and the procedure has a comparable fertility rate to myomectomy for women who want to conceive, according to what is thought to be the first study on the subject in the Middle East. The study was conducted by our group at Al Ain Hospital and presented ahead of print at the 2016 Arab Health Conference in Dubai, United Arab Emirates, in January and also presented at the Abu Dhabi annual gynecology conference in October 2015 and the Cleveland Clinic Abu Dhabi radiology conference in November 2015.
 Left uterine fibroid embolization in progress.
Left uterine fibroid embolization in progress.In this study, most women opted for UFE as a fertility treatment after failure of myomectomy or in vitro fertilization, or because hysterectomy was the only suggested option. Of the 210 patients who received UFE treatment, 35 women younger than the age of 40 wanted to conceive and had been unable.
Premature menopause, hysterectomy, and radiation exposures have been identified as barriers to fertility when treating women with UFE, and they might occur with other known UFE complications in a very small number of patients, less than 4%. However, uterine fibroids themselves rarely cause infertility, but they may be a causative factor of pregnancy loss. The study participants were advised to wait six months or more after UFE before attempting to conceive, of which the reported time range before attempting to conceive was seven to 33 months (average 20 months).
 Patient who became pregnant eight months post UFE. Obstetric third-trimester ultrasound images of a single fetus at age of 31 weeks 1 day and also at 34 weeks 1 day by last menstrual period (LMP). The previously embolized fibroid now measured 8.2 x 7.8 x 7.6 cm with degenerative changes. Placental localization is anterior with normal amniotic fluid. She delivered a full-term healthy baby by cesarian section.
Patient who became pregnant eight months post UFE. Obstetric third-trimester ultrasound images of a single fetus at age of 31 weeks 1 day and also at 34 weeks 1 day by last menstrual period (LMP). The previously embolized fibroid now measured 8.2 x 7.8 x 7.6 cm with degenerative changes. Placental localization is anterior with normal amniotic fluid. She delivered a full-term healthy baby by cesarian section.In a retrospective chart review of patients younger than the age of 40 (35 patients) who wished to spare their fertility and underwent UFE from 2011 to 2016, 18 patients reported 23 pregnancies, of which five were miscarriages. Two more pregnancies were complicated by premature labor. Of the 23 pregnancies, 16 were normal full-term pregnancies, 15 women had become pregnant once, and four had become pregnant twice.
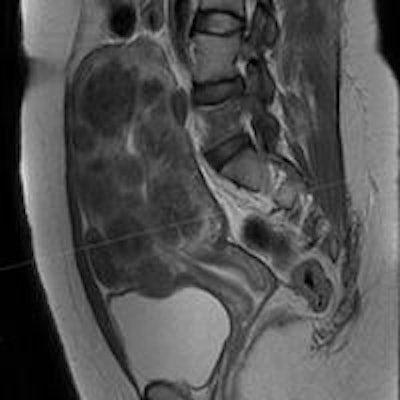
 Abdominal MR images showed a 30 x 20-cm single fibroid in a 34-year-old woman with severe menorrhagia and anemia. She was offered hysterectomy, but she opted to undergo UFE, which was successful in reducing the size by 60% and controlling her symptoms.
Abdominal MR images showed a 30 x 20-cm single fibroid in a 34-year-old woman with severe menorrhagia and anemia. She was offered hysterectomy, but she opted to undergo UFE, which was successful in reducing the size by 60% and controlling her symptoms.The remaining patients did not conceive. In the study, there was no reported intrauterine growth retardation in the prenatal period, fetal distress during labor, or problems related to uterine integrity. Two patients reported minor problems during pregnancy that were borderline oligohydramnios and low-lying placenta.
 MR image of the uterus in a 29-year-old woman showed multiple uterine fibroids in all locations, which was impossible to resect totally by surgery. This was an ideal UFE patient to save the uterus and fertility. Patient became pregnant 12 months after undergoing UFE.
MR image of the uterus in a 29-year-old woman showed multiple uterine fibroids in all locations, which was impossible to resect totally by surgery. This was an ideal UFE patient to save the uterus and fertility. Patient became pregnant 12 months after undergoing UFE.In the cohort of women who did conceive, overall, 16 out of 18 births proceeded normally without any complications (86%). Eight women delivered by cesarean section, and 10 women had normal vaginal delivery.
Our group of 23 pregnancies was small, but did confirm successful pregnancy after UFE. The 45.7% pregnancy rate in women younger than 40 years old who achieved a term pregnancy compares favorably with women who underwent myomectomy via a number of techniques. Of the women in the cohort who did conceive, subsequent birth proceeded normally (86%).
We compared this to abdominal myomectomy, in which the term pregnancy rate ranged from 10% to 46%, laparoscopic myomectomy (16% to 33%), and hysteroscopic mymomectomy (8% to 35%). This means the implications for uterine artery embolization as a primary treatment for uterine fibroids as a fertility-sparing technique is favorable. Our preliminary data suggest that fertility is further enhanced in women who underwent UFE as a first procedure to control uterine fibroids.
 MR images before and four months post UFE in a 32-year-old patient with a 5-cm submucosal fibroid. The patient's symptoms of pelvic pain and menorrhagia resolved one month post UFE. MRI showed significant reduction in the size of the submucosal fibroid and disappearance of ovarian cysts. This patient became pregnant six month post UFE.
MR images before and four months post UFE in a 32-year-old patient with a 5-cm submucosal fibroid. The patient's symptoms of pelvic pain and menorrhagia resolved one month post UFE. MRI showed significant reduction in the size of the submucosal fibroid and disappearance of ovarian cysts. This patient became pregnant six month post UFE.Significance of study
This study is significant, because it shows comparable fertility rates between the two primary uterus-sparing treatments widely available to treat fibroids: UFE and myomectomy, which is considered the gold standard for symptomatic fibroids in women who wish to conceive.
 The usual tools used for UFE: Robert catheter, microcatheter, and embolization particles.
The usual tools used for UFE: Robert catheter, microcatheter, and embolization particles.The results are surprising, because other old small studies have favored myomectomy over UFE for women who want to conceive. In this study of 210 women, UFE had a fertility rate of 47%. This is comparable to the fertility rate for myomectomy, which is 48%. The study proves that UFE not only allows women who were unable to conceive to become pregnant, but also allows them to have normal pregnancies with similar complication rates as the general population despite being a high-risk group. In the future, UFE will probably be a first-line treatment option even for women who wish to conceive and are unable due to the presence of uterine fibroids.
Given that myomectomy can be difficult in women with numerous interstitial and/or submucosal fibroids, and recurrence rates for fibroid tumors may be higher with myomectomy, UFE may provide a fertility-preserving alternative for some women.
Summary & conclusions
Pregnancy after UFE is well-documented. The risks of infertility following embolization, premature menopause, and hysterectomy are small, as is the radiation exposure during embolization. These risks compare favorably with those associated with myomectomy.
Fertility rates appear similar to patients undergoing myomectomy. No problems, either during pregnancy or delivery, have been observed after embolization. The course of pregnancy and delivery was normal after embolization with no major maternal or fetal complications reported. These findings confirm results from other centers that concluded that desire for future pregnancy is not a contraindication to fibroid embolization.
 Dr. Jamal Alkoteesh during an UFE procedure at Al Ain Hospital in the United Arab Emirates.
Dr. Jamal Alkoteesh during an UFE procedure at Al Ain Hospital in the United Arab Emirates.This was a small retrospective study based on patients being treated for fibroids by UFE in a single institution, and larger multicenter randomized prospective studies are needed comparing UFE and myomectomy.
For patients, the decision to undergo UFE if future pregnancy is desired is a complex one to make, and it should be made only after consultation with their gynecologist, an infertility specialist (if applicable), and an interventional radiologist.
Dr. Jamal Alkoteesh is the chief of interventional radiology and chairman of radiology at Al Ain Hospital in the United Arab Emirates, as well as an associate professor at United Arab Emirates University in Abu Dhabi. Dr. Alkoteesh is also a member of the Editorial Advisory Board of AuntMinnie.com's Middle East section.
The comments and observations expressed herein do not necessarily reflect the opinions of AuntMinnieEurope.com, nor should they be construed as an endorsement or admonishment of any particular vendor, analyst, industry consultant, or consulting group.

















