While the imaging community may be in agreement about the need to lower radiation doses in pediatric CT, the best way to do that is still up for debate. While some investigators concentrate on the calculations needed to deliver more precise doses, others work on refining the CT equipment itself. And all are concerned with maintaining superior image quality while doing what is safest for patients.
Four groups of researchers tackled this issue at the 2001 RSNA meeting. Austrian radiologists suggested that CT scanner dose calculation software generally underestimated organ radiation dose in pediatric patients, and offered a solution to this problem.
A team from Boston discussed optimized imaging protocols, while investigators from Vanderbilt University in Nashville looked into lowering mAs without distorting signal-to-noise ratio.
Finally, researchers from Germany showed how online tube-current modulation could cut back on radiation dose in multislice spiral CT exams.
CT dose index values
Dr. Stefan Puig and colleagues from the University of Vienna compared body CT dose index (CTDI) values provided by scanner manufacturers with CTDI values measured on phantoms simulating a pediatric patient.
Using a multislice CT scanner (Somatom Plus 4 Volume Zoom, Siemens Medical Solutions, Iselin, NJ) that automatically calculated CTDI values, the researchers scanned cylindrical polymethylmethacrylate (PMMA) phantoms with diameters between 0-32 cm, and calculated the CTDI values from dose measurements.
The team varied the tube voltage between 80, 120, and 140 kVp at 100 mAs to examine collimations of 0.5 mm, 1 mm, 2.5 mm, 5 mm, and 8 mm. The researchers found that body CTDI values given by CT scanner software underestimated the real organ dose in patients with a small body diameter. The CTDI values increased 30% from the CT-provided measurements when calculated with a 16-cm phantom. Without a phantom, the CTDI values increased up to 140% from the measurements given by the scanner software.
The increase was stronger for low kVp, but was nearly independent from the chosen collimation. At 120 kVp, absolute numbers for the CTDI measured in a 16-cm phantom increased from 0.122 mGy/mAs (4 x 5 mm) to 0.132 (4 x 2.5 mm) and 0.157 mGy/mAs (4 x 1 mm). With 80 kVp, the CTDI fell to 0.052 mGy/mAs for 4 x 1 mm collimation.
Optimized imaging protocol
In another study, Dr. Hamid Salamipour and colleagues from Massachusetts General Hospital in Boston sought to reduce radiation exposure by optimizing CT imaging protocols.
To optimize protocols of pediatric neck, chest, abdomen, and pelvis studies, the researchers reduced the mAs in three incremental stages, keeping the kVp constant. Salamipour and colleagues stratified the protocols for the patient’s age and weight.
The researchers enlisted two pediatric radiologists to interpret a random sampling of 632 images of pediatric patients on a scale of 1 to 3, where 1 meant unacceptable image quality, 2 indicated acceptable but inferior quality, and 3 signified undetectable loss of diagnostic image quality.

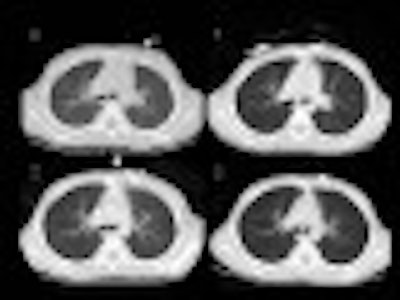
The MGH group reduced the mAs in incremental stages. In phase 0: kVp 120, mAs 210, pitch 1.0, slice thickness 5, calculated CTDIw 25. In phase 1: kVp 140, mAs 140, pitch 1.5, slice thickness 7, calculated CTDIw 23. In phase 2: kVp 140, mAs 130, pitch 1.5, slice thickness 5, calculated CTDIw 19. In phase 3: kVp 140, mAs 80, pitch 1.5, slice thickness 5, calculated CTDIw 12. Images courtesy of Dr. Hamid Salamipour. |
If the patient had undergone a previous CT study, the researchers asked the radiologists to compare the image quality of the research studies to that of the previous examination.
The researchers performed 331 of the 632 studies with a single-slice, helical CT scanner (HiSpeed, GE Medical Systems, Waukesha, WI). A GE LightSpeed Plus was used for scanning 301 patients. Weighted computer tomography dose index (CTDIw), as measured in 32-cm and 16-cm phantoms, was used to calculate the radiation doses of each scan within the three different imaging protocols.
The researchers found that the diagnostic quality of CT examinations performed with the lowest dose the researchers tested (mean 11.7 mGy, standard deviation 4.33, derivation 5.39) appeared virtually identical to the highest dose tested (mean 18 mGy, standard deviation 5.39). However, abdominal images produced at the lowest dose appeared somewhat grainy, Salamipour said.
Overall, radiation dose decreased 50% from the conventional protocol to the lowest-dose protocol. Conventional protocols for single-slice CT produced a radiation dose of 17.3 in single-slice CT and 31.4 in multislice CT. The lowest-dose protocols tested by the group resulted in radiation doses of 12.4 for single-slice CT and 16 for multislice CT.
Adjusted slice thickness
When mAs is reduced, so is the signal-to-noise ratio, and image degradation occurs. Dr. Marta Hernanz-Schulman from Vanderbilt University in Nashville, TN, set out to find another way to reduce radiation dose.
The team measured image signal-to-noise ratio, low-contrast lesion detection, and spatial resolution as a function of dose and slice thickness with a 16-cm low-contrast phantom.
The phantom was scanned at 120 kVp and 40 to 300 mAs in 20-mAs increments, with 3 mm, 5 mm, and 7 mm slice thicknesses at each level of mAs. The radiation dose ranged from 320 to 3,050 mrad at the phantom’s center. The phantom contained 13 lesions: one 22 mm and the rest 3-5 mm. Three pediatric radiologists, who were blinded to the image-acquisition data, reviewed the images.
"As you increase the mAs, particularly with the increased slice thickness, you significantly increase the number of lesions that are identified, which has a cut-point of about 160 mAs, below which there is no real difference in the number of lesions seen across each level of slice thickness," said Dr. Mark Reese, Hernanz-Schulman’s co-author.
Above 200 to 280 mAs, lesion detection decreased. The peak number of lesions detected at these mAs levels were 1 at 3 mm, 3.5 at 5 mm, and 5 at 7 mm.
When the researchers plotted the mean number of lesions detected against the signal-to-noise ratio, the results were roughly linear. At a 3-mm slice thickness, 0.49 lesions were detected, and at 7 mm, 0.69 lesions were detected. Spatial resolution remained constant at 71 lp/cm.
The researchers concluded that lesion detection depended upon mAs and slice thickness. Adjusting slice thickness and increasing mAs to approximately 160 maintains an acceptable signal-to-noise ratio, thereby reducing radiation exposure while keeping lesion detection constant.
Online tube-current modulation
In another presentation, Dr. Holger Greess and colleagues from the University of Erlangen-Nürnberg in Germany discussed the potential of online tube-current modulation in subsecond multislice spiral CT (MSCT) exams in 30 MSCT scans of the thorax and abdomen.
The team performed the exams on a Siemens Somatom Plus 4 Volume Zoom, with online tube-current control. This allowed tube-current modulation amplitude of up to 80% for 0.75 seconds.
Scan protocols for the thorax and abdomen used rotation times of 0.5 seconds, a slice collimation of 4 x 2.5 mm, a table feed of 15 mm per rotation (pitch 6), and 40 to 160 mAs.
Greess and colleagues evaluated mAs for tube-current modulation and compared it to the mAs in standard protocols. Three radiologists rated the image quality of the scans as either very good, good, or poor. The researchers assessed noise levels in comparison to a control group and by phantom measurements.
The researchers found that they could decrease radiation dose for noncircular patient cross-sections, without an increase in noise, if the tube current is reduced at angular positions in which the patient diameter and attenuation is small.
With online tube-current modulation, the researchers reduced the radiation dose of MSCT exams by 15%-30%, depending on patient geometry and anatomical region. The thorax scans showed a reduced radiation dose of 20%-30%, and the abdomen scans showed a reduced radiation dose of 15%-20%.
"Tube-current modulation has a strong potential to reduce patients’ dose. A mean reduction of 28% was observed over all scan regions," Greess said.
By Leslie FarnsworthAuntMinnie contributing writer
March 12, 2002
Related Reading
Chicago Children's Hospital lowers pediatric chest CT dose, November 29, 2001
Significant difference in radiation dose found between single- and multislice CT, November 25, 2001
FDA offers guidance on lowering CT dose, November 6, 2001
Study sparks fears over kids’ exposure to CT radiation, February 13, 2001
Copyright © 2002 AuntMinnie.com