CT and MR are both good at characterizing the morphology of cystic pancreatic masses, according to researchers at the University of California, San Francisco. The problem is with the masses themselves, which can appear benign when they aren't, and vice-versa.
"Cystic neoplasms of the pancreas present a unique diagnostic challenge to gastroenterologists, surgeons, and radiologists," said UCSF surgery resident Dr. Brendan Visser at the 2003 RSNA meeting. "They are increasingly being seen in CT scans, and there are increasing indications for resection. The consequences of mistaking a cystic neoplasm for a pseudocyst can be devastating," he said, noting that many patients are asymptomatic at presentation.
In an effort to determine the relative accuracy of CT and MR imaging for the presurgical characterization of such lesions as benign or malignant, Visser and colleagues performed a retrospective study of 58 patients (mean age 66, 2:1 ratio of men to women), all of whom had undergone either resection (50) or biopsy (8) of a cystic pancreatic mass between 1997 and 2003. In all there were 52 CT scans and 18 MRIs, for a total of 70 scans. Twelve patients underwent both MRI and CT.
"The images were interpreted by two dedicated abdominal radiologists who were blinded to all clinical data, and they were asked to evaluate the morphologic characteristics, as well as generate a differential diagnosis for each diagnosis on their list, as well as (rate) the overall probability of malignancy," Visser said. "A total of 23 morphologic characteristics were recorded for each scan."
Histopathology showed 10 mucinous cystadenomas, seven serous cystadenomas, seven mucinous cystadenocarcinomas, and eight pseudocysts, as well as four cystic ductal adenocarcinomas, four simple cysts, five intraductal papillary mucinous tumors, five cystic neuroendocrine tumors, and seven miscellaneous tumors. Twenty-one of 58 (36%) of the masses were malignant.
 |
| Serous cystadenoma with classic central, stellate calcification. All images courtesy of Dr. Brendan Visser. |
 |
| MRI shows multilocular serous cystadenoma (on T1 breath-hold the fine septations are visible). |
"For mass characterization as benign or malignant by reader, (reader 2), ROC analysis showed an area under the curve of 0.82 (0.76) for CT (p= 0.001 and 0.01, for readers 1 and 2, respectively) and 0.91 (0.85) for MR imaging (p=0.07 and 0.15)," Visser wrote in an e-mail to AuntMinnie.com.
 |
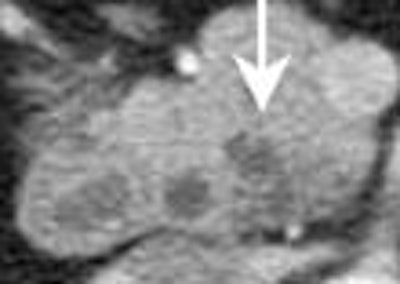
| Mucinous cystadenocarcinoma. Presence of mural calcifications (arrow) and septations are suggestive of malignancy. |
 |
| MRI demonstrating mucinous cystadenoma in tail of pancreas (arrow). On T2-weighted images the cyst fluid has high signal intensity similar to CSF. |
In fact, CT and MR results were quite similar, both in terms of predicting malignancy and in accuracy of diagnosis, he said.
But diagnostic accuracy was elusive with both modalities. The results showed that even when readers' confidence in the accuracy of their leading diagnosis rose to 90% or more, their diagnostic accuracy did not improve correspondingly, he said. In fact, in 40% of the cases, the two readers' leading diagnoses were identical, but that diagnosis was correct only 55% of the time.
 |
| Typical branch-duct intraductal papillary mucinous tumor in the uncinate seen on CT (left) and on MRI cross-section (middle) and coronal view (right). |
"We also investigated the standard criteria for benign periocystic, i.e. unilocular small, thin-walled lesions," Visser said. "Surprisingly, two of 13 or 15% of these were frankly malignant, another three were premalignant. This is a typical lesion, it appears relatively innocuous, it's a unilocular thin-walled lesion, but it turned out to be a mucinous cystadenocarcinoma." On the other hand, the intraductal papillary mucinous tumors were diagnosed with great accuracy.
Along with limitations due to the small sample size and the small number of cases that were imaged in both modalities (13), the study design invited selection bias, Visser said. First, there is significant bias inherent in choosing only pathologically proven lesions. Lesions that are characteristically very benign in appearance are often managed expectantly without surgery, he said, so only the suspect lesions would have made it into the study.
"The radiologists had a great deal of difficulty in distinguishing between pseudocysts and mucinous lesions, Visser added. "It's selection bias again because it isn't clear that (most) pseudocyst lesions end up in the operating room. Interestingly, four of those eight pseudocysts had been taken to the operating room because the surgeon preoperatively couldn't rule out cystadenoma. So there is also a selection bias in terms of operating on the ones that have a more similar appearance (to cystadenoma)."
MRI and CT demonstrate similar accuracy in differentiating malignant from premalignant or benign lesions, he said. "However, there is significant overlap (in) the morphologic characteristics...and an important limitation to both modalities is the substantial fraction of morphologically benign pancreatic masses that are in fact malignant."
Intraductal papillary mucinous tumors
In another study presented at the same session, Dr. Satomi Kawamoto and colleagues from Johns Hopkins Medical Center in Baltimore examined 36 consecutive patients who underwent preoperative four-slice contrast-enhanced MDCT prior to surgical resection and pathological diagnosis of intraductal papillary mucinous tumors, the type said to be the most easily diagnosed in the UCSF study.
The researchers administered contrast (120 ml at 3 ml/sec), and after a 25 and 50-60-second delays, acquired arterial and venous-phase images of the pancreas. The group assessed lesion morphology, the presence or absence of enhancement, and the probability of malignancy. All lesions seen at CT were compared with histopathological results following surgery.
Overall, CT detected 24 lesions (average maximum diameter 3.1 cm) in the pancreatic head and/or uncinate process, three in the head/neck region, five each in the body and tail, with diffuse multifocal involvement in four patients. There was pancreatic duct dilatation in 26 patients, including main and branch ducts in 22 patients, and branch duct in four. Ductal carcinoma in situ was found in nine patients, and invasive carcinoma in 15.
The head and uncinate process were the most common location of intraductal papillary mucinous tumors. Among the predictive factors in CT for malignancy were tumor size (p=0.002), the presence of contrast enhancement (p=0.0095), solid appearance (p<0.0001) and dilatation of more than 15 mm in the common bile duct at CT or presence of CBD stent (p=0.0007), the authors wrote in an accompanying abstract.
In addition, larger diameter of the main pancreatic duct was also correlated with presence of invasive carcinoma, which was also reported by other investigators at the session, Kawamoto wrote in an e-mail to AuntMinnie.com, noting that in her group's study, the invasive carcinomas were relatively large and therefore easily detected by CT.
"However, as other investigators reported, I think small invasive carcinomas and carcinoma in situ are still difficult to detect by imaging modalities," she wrote. "So our study can conclude CT is useful to predict invasive carcinoma for surgeons to plan surgical procedures, but does not exclude the need for further evaluation such as biopsy or surgery."
By Eric BarnesAuntMinnie.com staff writer
February 5, 2004
Related Reading
Mayo group seeks to optimize pancreatic MDCT protocols, October 27, 2003
Tumor marker useful in predicting pancreatic cancer resectability, October 2, 2003
High pitch, thin sections can optimize MDCT protocols, August 22, 2003
Ultrasound of the pancreas: what normal looks like, December 17, 2002
MRI with Teslascan preferred over CT for detection of pancreatic cancer, September 16, 2002
Copyright © 2004 AuntMinnie.com


















