A study from Harvard Medical School in Boston and the University of Aachen in Germany found substantial opportunities for dose reduction in CT coronary artery calcium scoring, particularly among smaller patients, and especially when calcium mass measurements are used instead of Agatston or volume scoring.
Perhaps more important, the group made a rare transition from acrylic phantoms to human subjects, using a noise-generating program to simulate multiple exposures in 20 patients who were scanned only once. The in-vivo results corresponded to those of the phantom study, suggesting that the superiority of the mass scoring method carries over to its use in patients.
"Coronary calcium scoring is a test that’s usually applied to asymptomatic individuals for stratification of cardiac risk," said Dr. Joseph Schoepf at the 2004 European Congress of Radiology in Vienna. "Since those people are a priori healthy, radiation doses should be kept to an absolute minimum in order not to overradiate those patients. Our goal…was to evaluate the accuracy of different coronary artery calcium scores and parameters for accurately measuring coronary artery calcium in different body types."
Phantom findings
The study was divided into two parts. First came experiments using an acrylic phantom specially designed for CT cardiac applications. The device was surrounded by fat-like extension rings representing small (30 cm), medium (35 cm), and large (40 cm) patients.
CT images were acquired with the aid of a 16-slice Somatom Sensation scanner (Siemens Medical Solutions, Malvern, PA), at 120 kVp and 50, 70, 90, 110, 130, 150, 170, and 190 effective mAs, respectively. At 80 kVp, data were acquired at 70, 100, 150, 200, 250, 300, 350, 400, and 450 mAs, respectively, using a retrospective ECG-gating protocol throughout. Agatston, Ca-volume and Ca-mass scores were obtained in each of 51 data sets, with the aid of a Siemens Leonardo workstation, Schoepf said.
"Radiation dose was measured in the phantom using (thermoluminescent) dosimeters within each region of interest," he said. "Variations in the calcium score for low-dose settings were compared to the standard dose. We assumed a variation of smaller than 10% from the baseline at full dose as acceptable in looking at the variability of calcium scores in actual patients. We know how variable those scores are."
For the phantom equivalent of small patients at 120 kVp, the scores were accurate at all mAs settings (50 mAs = 3 mGy).
"So if you have that small body type scanned at 120 kVp, you don’t need to scan with a radiation exposure of 2 mSv in men, but you can lower your radiation to 0.6 mSv," Schoepf said. "With a small body type all calcium scores are accurate. It’s also true at 80 kVp -- if you apply the margin of 10% above or below baseline, they all actually stay accurate. So you could in theory scan with 0.2 mSv effective radiation exposure in those patients."
For the phantom equivalent of medium patients, the variation passed the 10% threshold at <110 mAs (7.93 mGy) using the Agatston score, but remained accurate at all other mAs settings with calcium mass and volume. Reproducibility fell apart even sooner for the phantom equivalent of large patients: The variation was greater than 10% at <130 mAs (9.45 mGy) using Agatston, at <110 mAs using Ca-volume, and at <90 mAs (6.49 mGy) using Ca-mass. The calcium mass method enabled accurate scoring at 70 mAs or 1.62 mGy for the equivalent of small body types; at 100 mAs (2.32 mGy) for the equivalent of medium body types; and at <250 mAs (5.80 mGy) for the equivalent of large body types.
"There is significant interest in minimizing radiation exposure in coronary calcium scores with MDCT," he said. "For small body types, Agatston scores, volume scores, and mass scores remain stable and accurate over a broad range of standard tube-current settings, and that’s largely independent of the image noise. The radiation exposure can be significantly reduced while maintaining the accuracy of radiation dose measurements, by adapting the tube current to the body type. The calcium mass score appears to be the most robust vis-à-vis low radiation dose settings and the (corresponding) high level of image noise."
The human connection
Moving to the human portion of the study, Schoepf, along with colleagues Dr. Jens Martensen, Dr. Kelly Zou, Dr. Bernhard Schmidt, Dr. Stefaan Ulzheimer, and Willi Kalender, Ph.D., scanned 20 asymptomatic subjects using the same 16-slice Siemens scanner as used in the phantom study, at 120 kVp and at 170 mAs, and using a retrospective ECG gating protocol.
"Since you can’t scan those patients multiple times, we used a software platform to add artificial image noise," Schoepf said. The Vamp syngo Explorer application was applied to the resulting images to simulate reduced mAs of 150, 130, 110, 90, 70, and 50 in consistent regions of interest over the left ventricle. All three methods of calcium scoring were again applied in the usual manner at all noise degradation levels. Scoring variations at low-dose settings were again compared to those at the full dose, he said.
The software application has been shown to provide a realistic simulation of low-dose CT acquisitions, Schoepf wrote in an e-mail to AuntMinnie.com (Radiographics, March-April 2004, Vol. 24:2, pp. 601-13).
 |
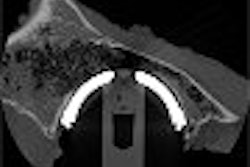
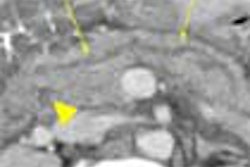
| Top, patient was scanned with 120 kVp/170 mAs. Below, artificial image noise was added using the Siemens Vamp syngo Explorer to simulate acquisition with lower dose settings at 120 kV/110mAs and 120kV/50 mAs. Calcifications in the left main coronary artery are highlighted in green, those in the left anterior descending coronary artery in yellow, and those in the left circumflex coronary artery in blue. The calcium scores at the three dose settings are not significantly different. Images courtesy of Dr. Joseph Schoepf. |
 |
 |
The 20 patients’ mean BMI was on the heavy side: 29.72. The average skin radiation dose -- at 120 kVp and 170 mAs including topogram -- was 11.13 mGy, for an effective radiation-dose equivalent of 1.97 mSv for men and 2.95 mSv for women. Using calcium mass measurements, the mean score was 170, in a well-distributed range from 0 to 1,775. Agatston scores ranged from 0 to 1,671.)
 |
| Results in 20 patients show that calcium mass offers less variability than Agatston or calcium volume measurements as image noise increases. Dose settings on the x-axis were adjusted by the simulation software; individual patient results and BMI were plotted separately for each calcium-scoring method. Chart courtesy of Dr. Joseph Schoepf. |
Commenting on additional charts that showed the accuracy of each scoring method broken down by patient and BMI, Schoepf said that while the Agatston method was accurate over the full range of radiation doses in slim subjects with a low body mass index (BMI 20-25), variation rose significantly in patients with higher body mass, as in the phantom study.
"If you apply the volume score instead of the Agatston score, the overall variability from baseline decreases from 95% to 55%," Schoepf said. "Even with the (larger-sized) group, body mass up to 45, you stay accurate over a broader range of scanner settings. And that's truer for the mass score, again the overall variability is much smaller (35%) as compared to the Agatston score and the volume score. This means that mass indices can be assessed accurately even with very low radiation doses."
The maximum variations at low-dose settings compared to baseline scores at full-dose scanning were 55% for the Agatston method, 30% for calcium volume and 13% for calcium mass. Image noise levels more than doubled with decreasing dose.
In conclusion, Schoepf said, adapting the tube current to the body mass index and body type of the patient offers significant opportunities for dose reduction -- "because measuring the calcium score is largely independent of the image noise." The calcium mass score was again the most robust method in the patient experiment, and can therefore be recommended for measuring coronary artery calcium, he said.
Asked to provide rough imaging guidelines for larger patients, Schoepf said it would be audacious to suggest protocols based solely on his group’s 20-patient study. However, specific protocols are being developed by the International Consortium for Standardization in Cardiac CT, he said, based on the diameter of the thorax rather than BMI, a similar approach.
The consortium is developing calibrations and protocols for a wide range of scanners, and radiologists will be able to obtain the information from the manufacturers as it becomes available for each scanner model. These calibrations will enable significant dose reductions, he said.
"The mass score seems to be the most robust simply because it’s based on a scanner-specific calibration, which allows you to play around with your radiation dose settings in a way that makes it independent of the scanner setting that’s actually used," Schoepf said. "That’s done once for the scanner and it stays with the protocol."
Session moderator Dr. Bernd Wintersperger from the University of Munich in Germany added that individualized scanner calibrations enable the modification of kVp settings in particular during imaging acquisition for calcium mass scoring; no such calibrations are needed to vary mAs.
"When you change the kV(p) settings, the Agatston score and volume score are out of the range of variability by about 20% to 30%," Wintersperger said. "With the mass score, individual calibration to different settings on the scanner is the only way to allow you to change protocols for different kV(p) settings, so this is the way you should all do calcium scoring."
By Eric Barnes
AuntMinnie.com staff writer
April 30, 2004
Related Reading
Radiologists correlate coronary calcium with other CVD markers, April 6, 2004
Patients shape up after viewing CT scans of their own blocked arteries, March 24, 2004
Accuracy of multidetector CT for coronary stenosis depends on patient selection, March 15, 2004
Coronary calcium scan gains ground as prognostic tool, August 6, 2003
Study finds blacks have less coronary calcium than whites, February 17, 2003
Copyright © 2004 AuntMinnie.com